

Standardised practices in the networked management of congenital hyperinsulinism: a UK national collaborative consensus
- PMID: 38027197
- PMCID: PMC10646160
- DOI: 10.3389/fendo.2023.1231043
Standardised practices in the networked management of congenital hyperinsulinism: a UK national collaborative consensus
Abstract
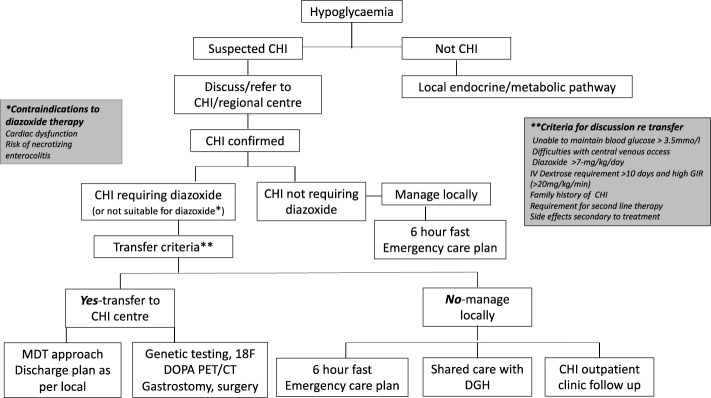
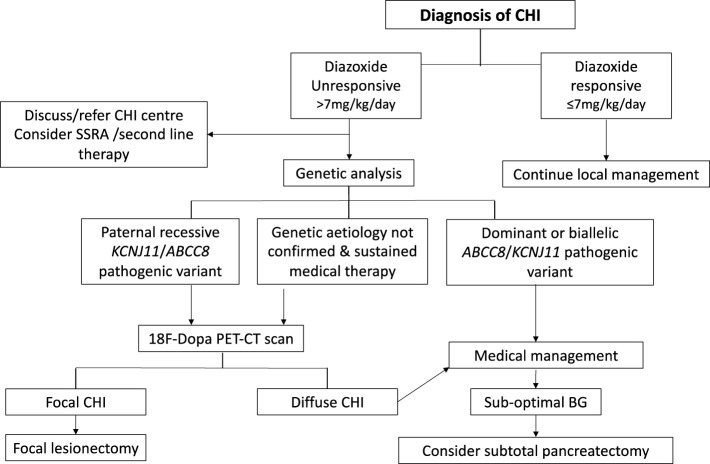
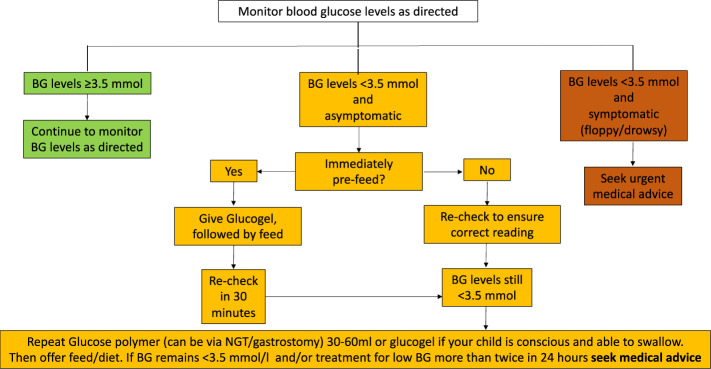
Congenital hyperinsulinism (CHI) is a condition characterised by severe and recurrent hypoglycaemia in infants and young children caused by inappropriate insulin over-secretion. CHI is of heterogeneous aetiology with a significant genetic component and is often unresponsive to standard medical therapy options. The treatment of CHI can be multifaceted and complex, requiring multidisciplinary input. It is important to manage hypoglycaemia in CHI promptly as the risk of long-term neurodisability arising from neuroglycopaenia is high. The UK CHI consensus on the practice and management of CHI was developed to optimise and harmonise clinical management of patients in centres specialising in CHI as well as in non-specialist centres engaged in collaborative, networked models of care. Using current best practice and a consensus approach, it provides guidance and practical advice in the domains of diagnosis, clinical assessment and treatment to mitigate hypoglycaemia risk and improve long term outcomes for health and well-being.
Keywords: congenital hyperinsulinism; consensus; glucose; hypoglycaemia; patient organisation; standardised practice; treatment.
Copyright © 2023 Shaikh, Lucas-Herald, Dastamani, Salomon Estebanez, Senniappan, Abid, Ahmad, Alexander, Avatapalle, Awan, Blair, Boyle, Chesover, Cochrane, Craigie, Cunjamalay, Dearman, De Coppi, Erlandson-Parry, Flanagan, Gilbert, Gilligan, Hall, Houghton, Kapoor, McDevitt, Mohamed, Morgan, Nicholson, Nikiforovski, O'Shea, Shah, Wilson, Worth, Worthington and Banerjee.
Conflict of interest statement
IB has received honoraria for advisory opinion from Merck and Diurnal Pharmaceuticals. He is the UK CI for clinical trials funded by Zealand Pharmaceuticals and has received grant funding from Merck, Diurnal and Crinetics Pharmaceuticals. IB is the Chair of the BSPED-NIHR Clinical Studies Group and the Chair of the ESPE Communications Committee. He is a co-opted member of the NICE Head Injury Update Committee. IB has advisory roles with several patient organisations including the Pituitary Foundation, Living with CAH, CHC and CHI. MGS has received funding/speaker honorium from Novo Nordisk, Sandoz, Pfizer and received honorarium for consultancies/advisory boards from Novo Nordisk, Pfizer and Merck. RK has received grant funding and honoraria for advisory opinion from Merck. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources