

Predictors of Postdeployment Functioning in Combat-Exposed U.S. Military Veterans
- PMID: 38027424
- PMCID: PMC10663646
- DOI: 10.1177/2167702617703436
Predictors of Postdeployment Functioning in Combat-Exposed U.S. Military Veterans
Abstract
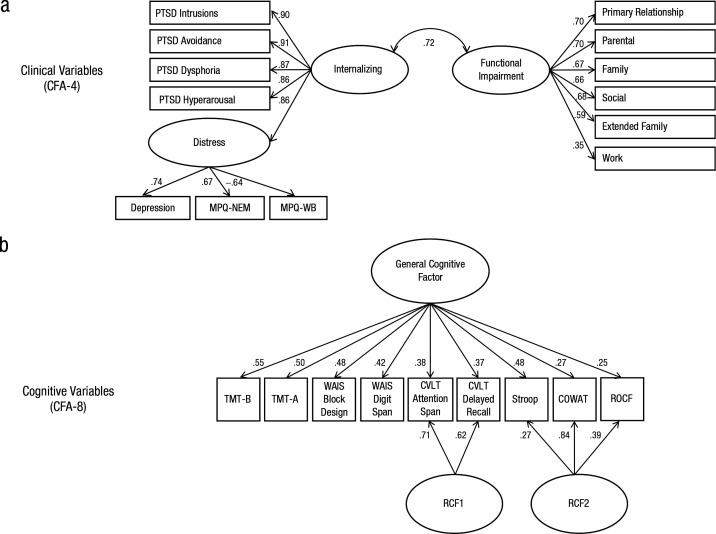
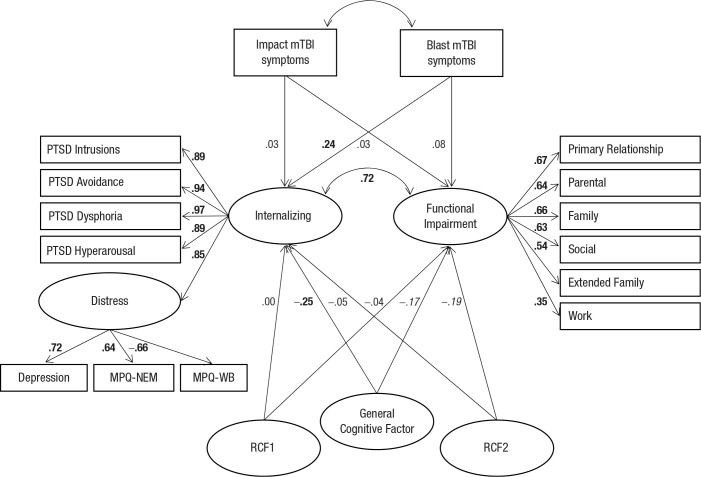
Posttraumatic stress disorder (PTSD) and sequelae of mild traumatic brain injury (mTBI) are presumed to contribute to reintegration difficulties in combat-exposed veterans. Yet their relative impacts on postdeployment functioning are not well understood. The current study used structural equation modeling (SEM) to clarify the extent to which symptoms of internalizing disorders (e.g., depression, anxiety), mTBI symptoms, and cognitive performance are associated with functional impairment in 295 combat-exposed veterans. SEM results showed that internalizing symptoms most significantly predicted functional impairment (r = 0.72). Blast mTBI and cognitive performance were associated with internalizing (r = 0.24 and -0.25, respectively), but functional impairment was only modestly related to cognition (r = -0.17) and unrelated to mTBI. These results indicate that internalizing symptoms are the strongest predictor of functioning in trauma-exposed veterans, exceeding the effects of mTBI and cognitive performance. This evidence supports prioritizing interventions that target internalizing psychopathology to improve functioning in cases of co-occurring PTSD and mTBI.
Keywords: neuropsychology; posttraumatic stress disorder; trauma; war.
© The Author(s) 2017.
Conflict of interest statement
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
Figures
References
-
- American Psychiatric Association. (2000). Diagnostic criteria from DSM-IV-TR. Arlington, VA: American Psychiatric Association.
-
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing.
-
- Antshel K. M., Faraone S. V., Maglione K., Doyle A. E., Fried R., Seidman L. J., Biederman J. (2010). Executive functioning in high-IQ adults with ADHD. Psychological Medicine, 40(11), 1909–1918. http://doi.org/S0033291709992273 - PubMed
-
- Arbisi P. A., Polusny M. A., Erbes C. R., Thuras P., Reddy M. K. (2011). The Minnesota Multiphasic Personality Inventory–2 Restructured Form in National Guard soldiers screening positive for posttraumatic stress disorder and mild traumatic brain injury. Psychological Assessment, 23(1), 203. 10.1037/a0021339 - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials