

The emerging role of digital health in the management of asthma
- PMID: 38028951
- PMCID: PMC10657529
- DOI: 10.1177/20406223231209329
The emerging role of digital health in the management of asthma
Abstract
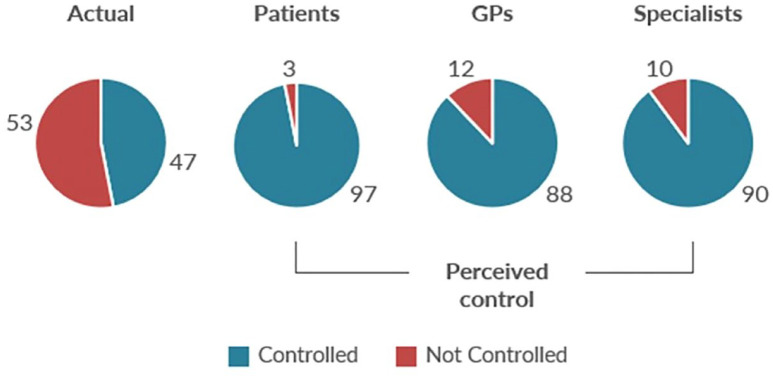
The most common reasons seen for lack of asthma control include misconceptions about disease control, low controller treatment adherence, poor inhaler technique, and the resulting underuse of controllers and overuse of short-acting beta2 agonists (SABAs). Narrowing these care gaps may be achieved through well-designed patient education that considers the patient's motivation, beliefs, and capabilities regarding their asthma and its management and empowers the patient to become an active participant in treatment decisions. Digital health technologies (DHTs) and digital therapeutic (DT) devices provide new opportunities to monitor treatment behaviors, improve communication between healthcare providers and patients, and generate data that inform educational interactions. DHT and DT have been proven effective in enhancing patient self-management in other chronic conditions, particularly diabetes. Accelerated integration of DHT and DT into the management of asthma patients is facilitated by the use of digital inhalers that employ sensor technology ("smart" inhalers). These devices efficiently provide real-time feedback on controller adherence, SABA use, and inhaler technique that have the strong potential to optimize asthma control.
Keywords: adherence; asthma; digital health technology; disease control; health outcomes; inhaler technique; patient education; patient engagement; patient-provider communications; smart inhaler.
© The Author(s), 2023.
Conflict of interest statement
Dr. AK declares that he has received consulting fees from AstraZeneca, Bellus, Covis Pharma, Eisai, GlaxoSmithKline, Pfizer, Merck Frost, Sanofi, Teva, Trudel, and Valeo. He has received honoraria from AstraZeneca, Boehringer Ingelheim, Covis Pharma, Cipla, Eisai, GlaxoSmithKline, Merck Frosst, Novo Nordisk, Moderna, Pfizer, Sanofi, Teva, Trudel, and Valeo. He received a FENO machine from Sanofi as part of a severe asthma survey. Mr. MB declares that he has received honoraria as a speaker and consultant for CHE activities from Pfizer, Novo Nordisk, Khiron, Johnson & Johnson, AbbVie, Teva, Biosyent, Boehringer Ingelheim, Moderna, Canopy, and Valneva. He has also been a consultant for CHE activities on advisory boards for Novo Nordisk, Emergent BioSolutions, Pfizer, and Novamax. Dr. JB declares that he has no competing interests in association with this manuscript. Dr. JK declares that he received grants/contracts from Novo Nordisk. He received consulting fees from Abbott, AbbVie, AstraZeneca, Bayer, BD, Boerhinger Ingelheim, Eisai, Embecta, Eli Lilly, GlaxoSmithKline, Janssen, Novo Nordisk, Miravo Pharm, Teva, Takeda, and Sanofi. He has received honoraria from Abbott, AbbVie, AstraZeneca, Boerhinger Ingelheim, Eisai, Embecta, Eli Lilly, GlaxoSmithKline, Janssen, Novo Nordisk, Miravo Pharm, Moderna, Pfizer Takeda, Sanofi, and Otsuka. Dr. SH declares that he received an honorarium as a workshop facilitator for Teva. Dr. CL declares that his institution has received grants/contracts from AstraZeneca, the Ontario Ministry of Health, Canadian Institutes of Health Research, and the Federal Economic Development Agency for Southern Ontario. His company has received payment/honoraria from AstraZeneca, Boerhinger Ingelheim, Covis Pharma, GlaxoSmithKline, Novartis, and Valeo. He has participated in advisory boards for AstraZeneca, GlaxoSmithKline, Novartis, Sanofi Genzyme, and Teva.
Figures
References
-
- Racine G, Forget A, Moullec G, et al. Predictors of asthma control and exacerbations: a real-world study. J Allergy Clin Immunol Pract 2021; 9: 2802–2811.e2. - PubMed
-
- Haselkorn T, Fish JE, Zeiger RS, et al. Consistently very poorly controlled asthma, as defined by the impairment domain of the Expert Panel Report 3 guidelines, increases risk for future severe asthma exacerbations in The Epidemiology and Natural History of Asthma: Outcomes and Treatment Regimens (TENOR) study. J Allergy Clin Immunol 2009; 124: 895–902.e1-4. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
