

Subcutaneous Infliximab in Refractory Crohn's Disease Patients: A Possible Biobetter?
- PMID: 38028954
- PMCID: PMC10640858
- DOI: 10.1093/crocol/otad040
Subcutaneous Infliximab in Refractory Crohn's Disease Patients: A Possible Biobetter?
Abstract
Background: A subcutaneous formulation of infliximab (IFX-SC) approved to treat patients with inflammatory bowel disease may offer improved efficacy versus intravenous infliximab.
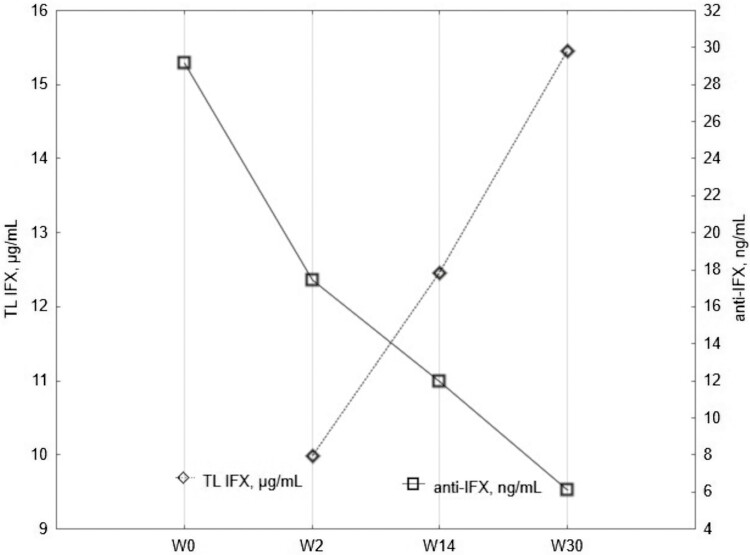
Methods: Patients with refractory Crohn's disease (CD, n = 32) previously treated unsuccessfully with at least 2 biologics were treated with IFX-SC and followed from baseline at Week 0 (W0) to Week 30 (W30). The study's primary endpoint was the treatment's persistence at W30, while secondary goals included the analysis of serum infliximab trough levels (TL IFX), dynamics of anti-IFX antibodies (ATIs), and clinical, serum and fecal markers of CD activity during IFX-SC treatment.
Results: Midterm treatment persistence with the continuation of treatment after W30 was 53%. TL IFX median values showed rapid, significant upward dynamics and exceeded 15.5 μg/mL at W30, whereas median ATI levels significantly declined. Among ATI-negative patients at W0 (n = 15), only one showed IFX immunogenicity with newly developed ATIs at W30. Among ATI-positive patients at W0, ATI seroconversion from ATI-positive to ATI-negative status was observed in 10 of 17 patients (58.8%). Patients who had continued IFX-SC treatment at W30 showed significant decreases in C-reactive protein (P = .0341), fecal calprotectin (P = .0002), and Harvey-Bradshaw index (P = .0029) since W0.
Conclusions: Patients with refractory CD previously treated with at least 2 biologics exhibited clinically relevant improvement with IFX-SC, which showed less immunogenic potential than IFX-IV and highly stable TL IFX.
Keywords: Crohn’s disease; Inflammatory bowel disease; antibodies to infliximab; immunogenicity; infliximab; infliximab trough levels; subcutaneous; treatment persistence.
© The Author(s) 2023. Published by Oxford University Press on behalf of Crohn's & Colitis Foundation.
Conflict of interest statement
K.C.: has consulted for Celltrion and Biogen. D.D.: has consulted for Takeda, AbbVie, Pfizer, and Janssen. M.L.: has consulted for Takeda and Pfizer. M.K.: has consulted for Pfizer. N.M.: has consulted for Takeda and Janssen. V.H.: has consulted for Biogen and Janssen. K.M.: has consulted for Takeda and Janssen. K.K.: has consulted for Abbott. M.K.: has consulted for Takeda and Janssen. J.J.: none. K.K.: none. G.V.: none. S.P.: none. M.L.: provided consultations and received fees for lectures by Celltrion, Abbvie, Janssen, Takeda, and Ferring.
Figures


References
-
- D’Amico F, Solitano V, Aletaha D, et al. Biobetters in patients with immune-mediated inflammatory disorders: an international Delphi consensus. Autoimmun Rev. 2021;20(7):102849. - PubMed
-
- Alten R, An Y, Kim DH, Yoon SW, Peyrin-Biroulet L.. Re-routing infliximab therapy: subcutaneous infliximab opens a path towards greater convenience and clinical benefit. Clin Drug Investig. 2022;42(6):477-489. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials