

Untreated cervical intraepithelial neoplasia grade 2 and subsequent risk of cervical cancer: population based cohort study
- PMID: 38030154
- PMCID: PMC10685285
- DOI: 10.1136/bmj-2023-075925
Untreated cervical intraepithelial neoplasia grade 2 and subsequent risk of cervical cancer: population based cohort study
Abstract
Objective: To describe the long term risk of cervical cancer in women with untreated (that is, undergoing active surveillance) or immediately treated cervical intraepithelial neoplasia grade 2 (CIN2).
Design: Nationwide population based historical cohort study.
Setting: Danish healthcare registries.
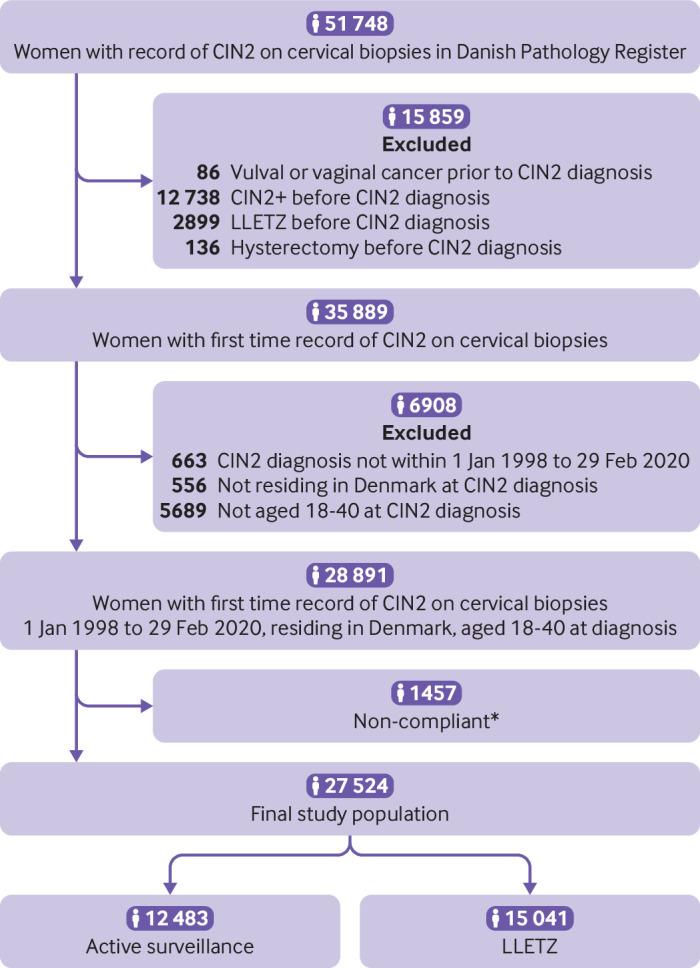
Participants: Women with CIN2 diagnosed in 1998-2020 and aged 18-40 years at diagnosis, who had either active surveillance or immediate treatment with large loop excision of the transformation zone (LLETZ). Women with a previous record of CIN2 or worse or LLETZ were excluded.
Main outcome measure: A Weibull survival model for interval censored time-to-event data was used to estimate the cumulative risk of cervical cancer. Inverse probability treatment weighting was used to adjust estimates for age, index cytology, calendar year, and region of residence.
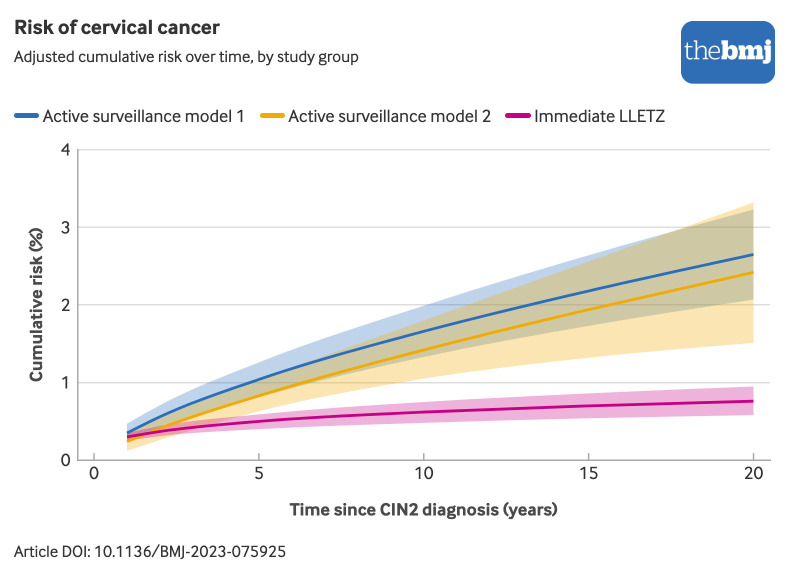
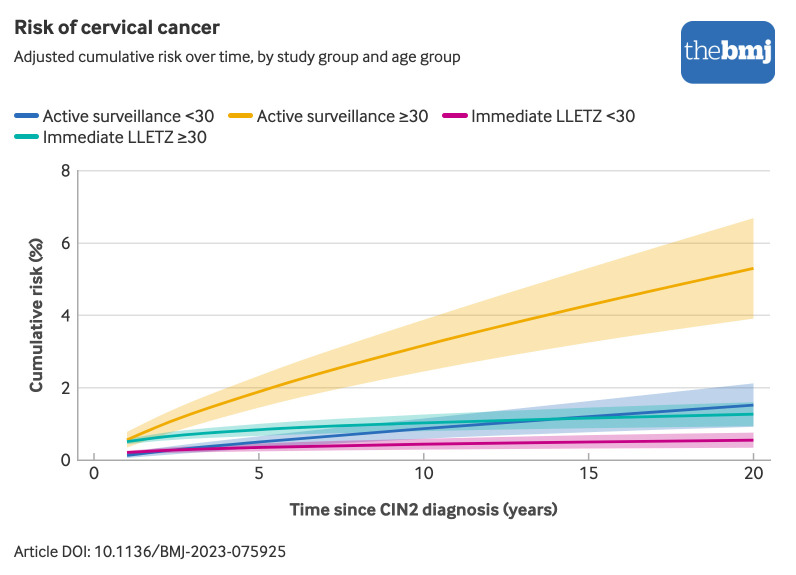
Results: The cohort included 27 524 women with CIN2, of whom 12 483 (45%) had active surveillance and 15 041 (55%) had immediate LLETZ. During follow-up, 104 cases of cervical cancer were identified-56 (54%) in the active surveillance group and 48 (46%) in the LLETZ group. The cumulative risk of cervical cancer was comparable across the two groups during the active surveillance period of two years. Thereafter, the risk increased in the active surveillance group, reaching 2.65% (95% confidence interval 2.07% to 3.23%) after 20 years, whereas it remained stable in the LLETZ group at 0.76% (0.58% to 0.95%).
Conclusions: Undergoing active surveillance for CIN2, thereby leaving the lesion untreated, was associated with increased long term risk of cervical cancer compared with immediate LLETZ. These findings show the importance of continued follow-up of women having active surveillance.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at https://www.icmje.org/disclosure-of-interest/ and declare: support from the Danish Cancer Society, Central Region Denmark, Carpenter Axel Kastrup-Nielsen’s Memorial Fund, Manufacturer Einar Willumsen’s Memorial Fund, and Merchant AV Lykfeldt’s Grant; KDL has received a speaker’s fee from AstraZeneca; RKD and AH have received reagents at reduced cost from Roche Denmark; LP has received a speaker’s fee from MSD; no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Athanasiou A, Veroniki AA, Efthimiou O, et al. Comparative effectiveness and risk of preterm birth of local treatments for cervical intraepithelial neoplasia and stage IA1 cervical cancer: a systematic review and network meta-analysis. Lancet Oncol 2022;23:1097-108. 10.1016/S1470-2045(22)00334-5 - DOI - PMC - PubMed