

Relationship between initial red cell distribution width and ΔRDW and mortality in cardiac arrest patients
- PMID: 38030411
- PMCID: PMC10804170
- DOI: 10.1002/ehf2.14602
Relationship between initial red cell distribution width and ΔRDW and mortality in cardiac arrest patients
Abstract
Aims: There has been a lack of research examining the relationship between red cell distribution width (RDW) and the prognosis of cardiac arrest (CA) patients. The prognostic value of the changes in RDW during intensive care unit (ICU) hospitalization for CA patients has not been investigated. This study aims to investigate the correlation between RDW measures at ICU admission and RDW changes during ICU hospitalization and the prognosis of CA patients and then develop a nomogram that predicts the risk of mortality of these patients.
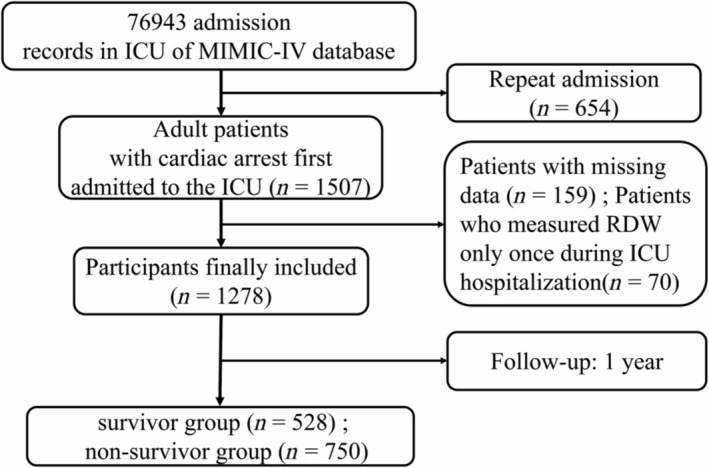
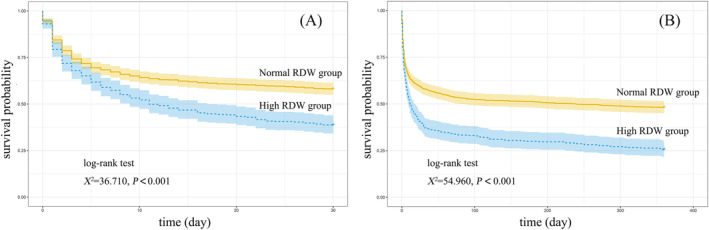
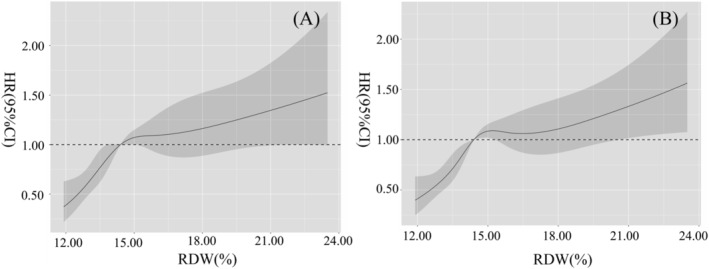
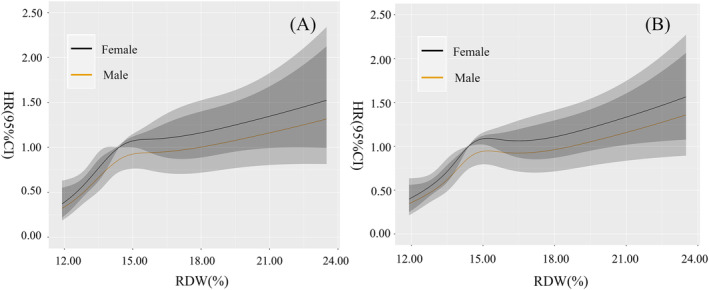
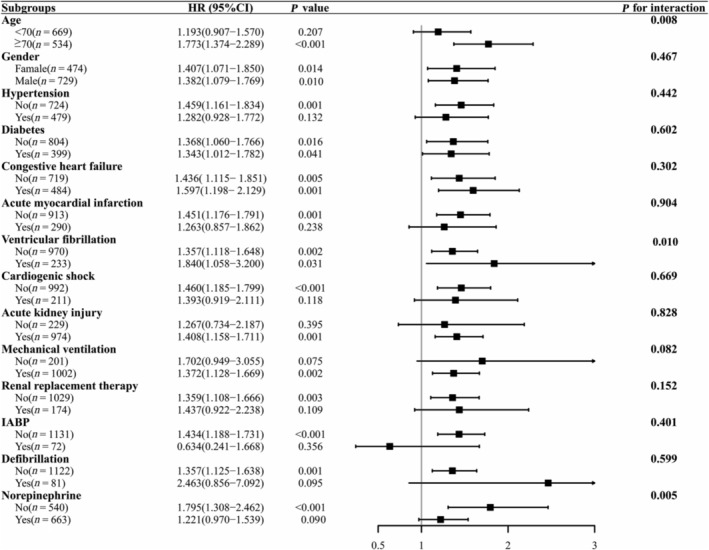
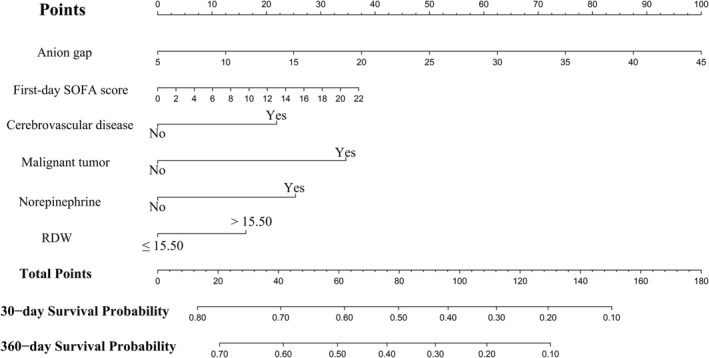
Methods and results: A retrospective cohort study is used to collect clinical characteristics of CA patients (>18 years) that are on their first admission to ICU with RDW data measured from the Medical Information Mart for Intensive Care IV Version 2.0 database. Patients are randomly divided into a development cohort (75%) and a validation cohort (25%). The primary outcome is 30 and 360 day all-cause mortality. ΔRDW is defined as the RDW on ICU discharge minus RDW on ICU admission. A multivariate Cox regression model is applied to test whether the RDW represents an independent risk factor that affects the all-cause mortality of these patients. Meanwhile, the dose-response relationship between the RDW and the mortality is described by restricted cubic spine (RCS). A prediction model is constructed using a nomogram, which is then assessed using receiver operating characteristic curves, calibration curves, and decision curve analysis (DCA). A total of 1278 adult CA patients are included in this study. We found that non-survivors have a higher level of RDW and ΔRDW compared with survivors, and the mortality rate is higher in the high RDW group than in the normal RDW group. The Kaplan-Meier survival curve indicates that patients in the normal RDW group had a higher cumulative survival rate at 30 and 360 days than those in the high RDW group (log-rank test, χ2 = 36.710, χ2 = 54.960, both P values <0.05). The multivariate Cox regression analysis shows that elevated RDW at ICU admission (>15.50%) is an independent predictor of 30 [hazard ratio = 1.451, 95% confidence interval (CI) = 1.181-1.782, P < 0.001] and 360 day (hazard ratio = 1.393, 95% CI = 1.160-1.671, P < 0.001) all-cause mortality among CA patients, and an increase in RDW during ICU hospitalization (ΔRDW ≥ 0.4%) can serve as an independent predictor of mortality among these patients. A non-linear relationship between the RDW measured at ICU admission and the increased risk of mortality rate of these patients is shown by the RCS. This study established and validated a nomogram based on six variables, anion gap, first-day Sequential Organ Failure Assessment score, cerebrovascular disease, malignant tumour, norepinephrine use, and RDW, to predict mortality risk in CA patients. The consistency indices of 30 and 360 day mortality of CA patients in the validation cohort are 0.721 and 0.725, respectively. The nomogram proved to be well calibrated in the validation cohort. DCA curves indicated that the nomogram provided a higher net benefit over a wide, reasonable range of threshold probabilities for predicting mortality in CA patients and could be adapted for clinical decision-making.
Conclusions: Elevated RDW levels on ICU admission and rising RDW during ICU hospitalization are powerful predictors of all-cause mortality for CA patients at 30 and 360 days, and they can be used as potential clinical biomarkers to predict the bad prognosis of these patients. The newly developed nomogram, which includes RDW, demonstrates high efficacy in predicting the mortality of CA patients.
Keywords: Cardiac arrest; Cohort study; Intensive care unit; Mortality; Nomogram; Red cell distribution width.
© 2023 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
None declared.
Figures
Similar articles
-
[Development and validation of a prognostic model for patients with sepsis in intensive care unit].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023 Aug;35(8):800-806. doi: 10.3760/cma.j.cn121430-20230103-00003. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023. PMID: 37593856 Chinese.
-
Association Between the Red Blood Cell Distribution Width and 30-Day Mortality in Intensive Care Patients Undergoing Cardiac Surgery: A Retrospective Observational Study Based on the Medical Information Mart for Intensive Care-IV Database.Ann Lab Med. 2024 Sep 1;44(5):401-409. doi: 10.3343/alm.2023.0345. Epub 2024 Mar 12. Ann Lab Med. 2024. PMID: 38469636 Free PMC article.
-
Prognostic significance of increased preoperative red cell distribution width (RDW) and changes in RDW for colorectal cancer.Cancer Med. 2023 Jun;12(12):13361-13373. doi: 10.1002/cam4.6036. Epub 2023 May 4. Cancer Med. 2023. PMID: 37143237 Free PMC article.
-
Red blood cell distribution width at admission and the short-term mortality of patients with severe burn injury: a meta-analysis.Eur J Med Res. 2024 Dec 18;29(1):589. doi: 10.1186/s40001-024-02165-z. Eur J Med Res. 2024. PMID: 39696510 Free PMC article.
-
The prognostic value of red blood cell distribution width for mortality in intracranial hemorrhage: A systematic review and meta-analysis.Medicine (Baltimore). 2025 Mar 14;104(11):e41487. doi: 10.1097/MD.0000000000041487. Medicine (Baltimore). 2025. PMID: 40101061 Free PMC article.
References
MeSH terms
Grants and funding
- 2019C03024/Key Research and Development Plan of Zhejiang Province
- WKJ-ZJ-1811/Provincial and Ministerial Joint Construction of Key Projects of Zhejiang Medical and Health Science and Technology Plan
- 2022GY20/Science and Technology Program of Huzhou
- 2023KY314/Medical and Health Science and Technology Project of Zhejiang Province
- LGD20H150001/Basic Public Welfare Research Program of Zhejiang Province
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
