

Time-Varying Determinants of Graft Failure in Pediatric Kidney Transplantation in Europe
- PMID: 38030557
- PMCID: PMC10937011
- DOI: 10.2215/CJN.0000000000000370
Time-Varying Determinants of Graft Failure in Pediatric Kidney Transplantation in Europe
Abstract
Background: Little is known about the time-varying determinants of kidney graft failure in children.
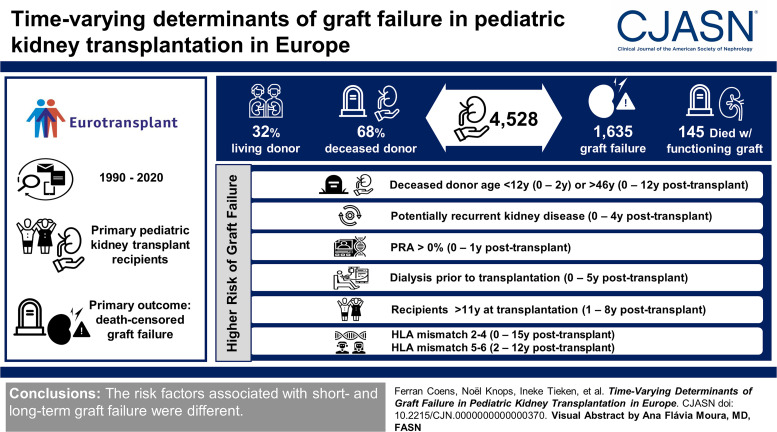
Methods: We performed a retrospective study of primary pediatric kidney transplant recipients (younger than 18 years) from the Eurotransplant registry (1990-2020). Piece-wise exponential additive mixed models were applied to analyze time-varying recipient, donor, and transplant risk factors. Primary outcome was death-censored graft failure.
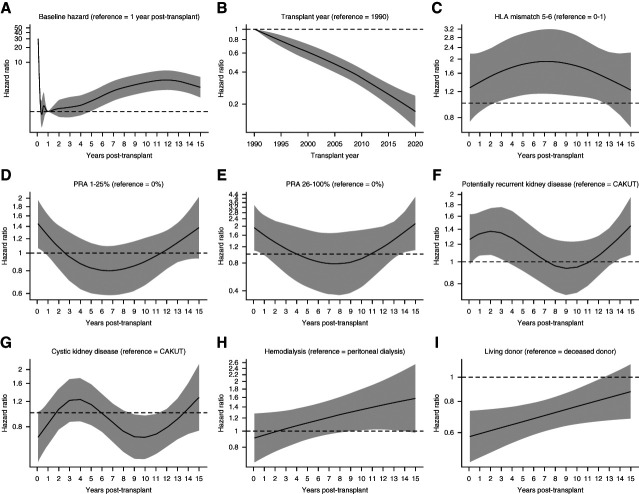
Results: We report on 4528 kidney transplantations, of which 68% with deceased and 32% with living donor. One thousand six hundred and thirty-eight recipients experienced graft failure, and 168 died with a functioning graft. Between 2011 and 2020, the 5-year graft failure risk was 10% for deceased donor and 4% for living donor kidney transplant recipients. Risk of graft failure decreased five-fold from 1990 to 2020. The association between living donor transplantation and the lower risk of graft failure was strongest in the first month post-transplant (adjusted hazard ratio, 0.58; 95% confidence interval, 0.46 to 0.73) and remained statistically significant until 12 years post-transplant. Risk factors for graft failure in the first 2 years were deceased donor younger than 12 years or older than 46 years, potentially recurrent kidney disease, and panel-reactive antibody >0%. Other determinants of graft failure included dialysis before transplantation (until 5 years post-transplant), human leukocyte antigen mismatch 2-4 (0-15 years post-transplant), human leukocyte antigen mismatch 5-6 (2-12 years post-transplant), and hemodialysis (8-14 years post-transplant). Recipients older than 11 years at transplantation had a higher risk of graft failure 1-8 years post-transplant compared with other age groups, whereas young recipients had a lower risk throughout follow-up. Analysis of the combined effect of post-transplant time and recipient age showed a higher rate of graft failure during the first 5 years post-transplant in adolescents compared with young transplant recipients. In contrast to deceased donor younger than 12 years, deceased donor older than 46 years was consistently associated with a higher graft failure risk.
Conclusions: We report a long-term inverse association between living donor kidney transplantation and the risk of graft failure. The determinants of graft failure varied with time. There was a significant cumulative effect of adolescence and time post-transplant. The ideal donor age window was dependent on time post-transplant.
Copyright © 2023 by the American Society of Nephrology.
Conflict of interest statement
J.J. Kim acknowledges funding from a MRC NIHR fellowship (MR/V037900/1). N. Knops reports research funding from Sandoz. L. Pape reports consultancy for Alexion, Alnylam, Chiesi, Neovii, and Novartis; research funding from Chiesi, Germany; and honoraria from Alexion and Chiesi. A. Prytula reports research funding from Astellas and Novo Nordisk. I. Tieken reports other interests or relationships with Eurotransplant. B. Toenshoff reports consulting fees from Bristol-Myers Squibb, Chiesi, CSL Behring Biotherapies for Life, and Vifor; research grants from Astellas, Chiesi, and Novartis; and participation in advisory boards of Bristol-Myers Squibb, Chiesi, and Vifor. S. Vogelaar reports employment with Eurotransplant International. Cooperative European Paediatric Renal TransplAnt INitiative (CERTAIN) registry acknowledges financial contribution from the Dietmar Hopp Stiftung, the European Society for Pediatric Nephrology (ESPN), the German Society for Pediatric Nephrology (GPN), and by grants from the pharmaceutical companies Astellas and Novartis. All remaining authors have nothing to disclose.
Figures



Comment in
-
Embracing Complexity to Better Serve Pediatric Kidney Transplant Recipients.Clin J Am Soc Nephrol. 2024 Mar 1;19(3):286-288. doi: 10.2215/CJN.0000000000000432. Epub 2024 Feb 5. Clin J Am Soc Nephrol. 2024. PMID: 38319991 Free PMC article. No abstract available.
References
-
- Chesnaye NC van Stralen KJ Bonthuis M, et al. .. The association of donor and recipient age with graft survival in paediatric renal transplant recipients in a European Society for Paediatric Nephrology/European Renal Association-European Dialysis and Transplantation Association Registry study. Nephrol Dial Transplant. 2017;32(11):1949–1956. doi:10.1093/ndt/gfx261 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
