

PD-1- CD45RA+ effector-memory CD8 T cells and CXCL10+ macrophages are associated with response to atezolizumab plus bevacizumab in advanced hepatocellular carcinoma
- PMID: 38030622
- PMCID: PMC10687033
- DOI: 10.1038/s41467-023-43381-1
PD-1- CD45RA+ effector-memory CD8 T cells and CXCL10+ macrophages are associated with response to atezolizumab plus bevacizumab in advanced hepatocellular carcinoma
Abstract
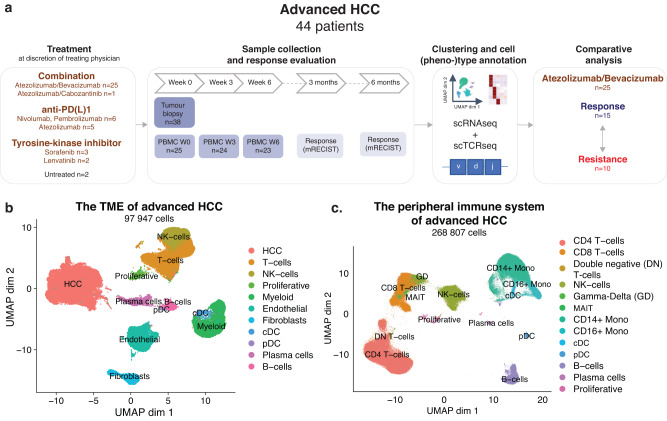
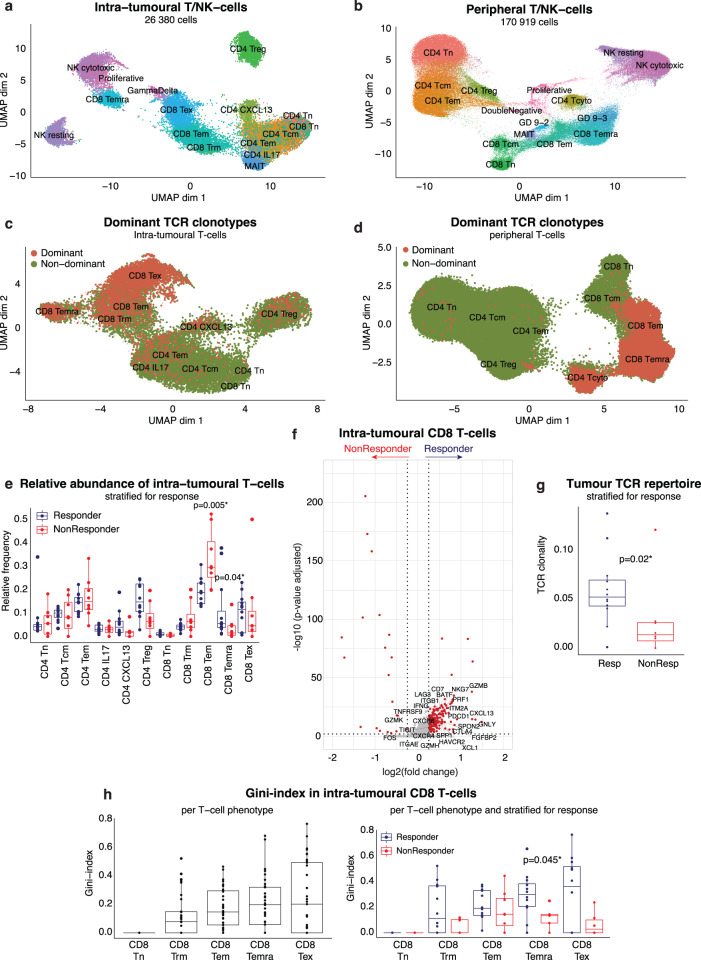
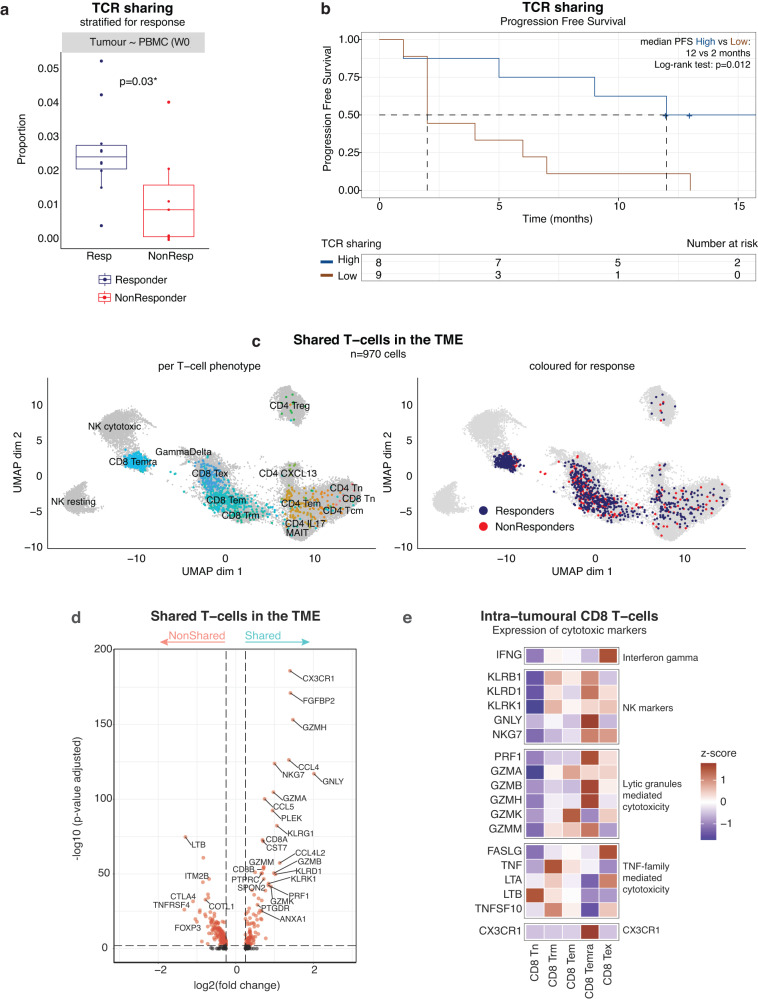
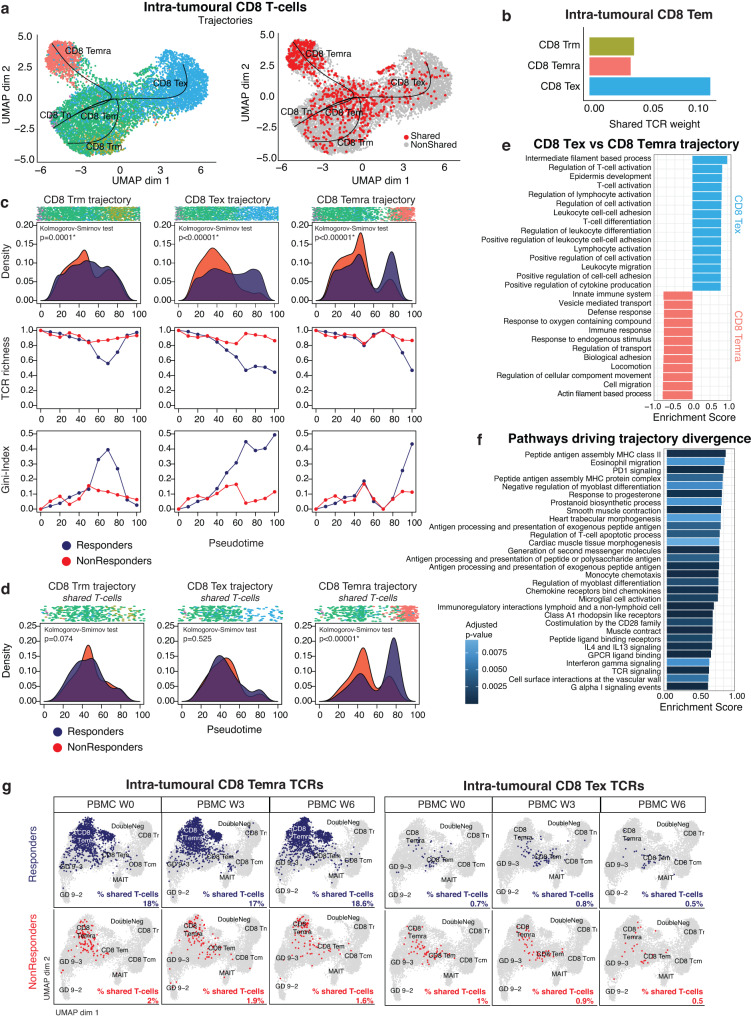
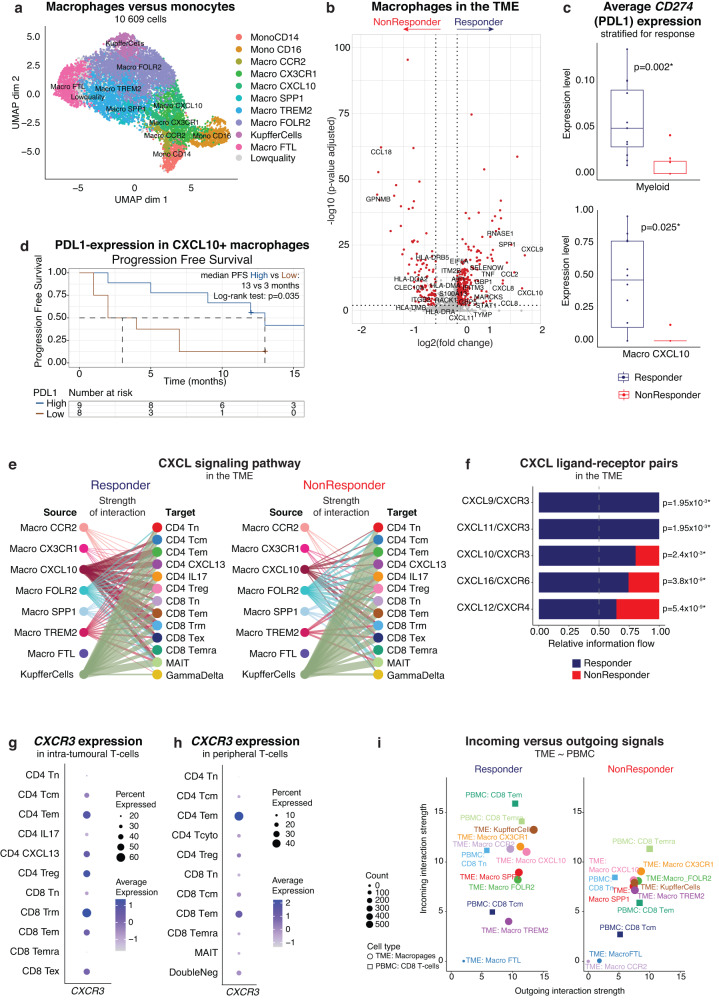
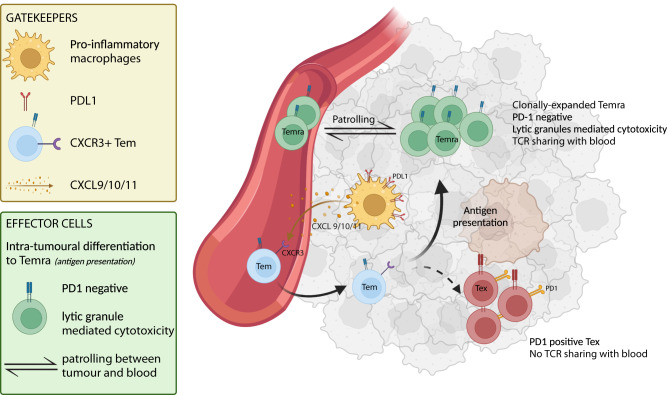
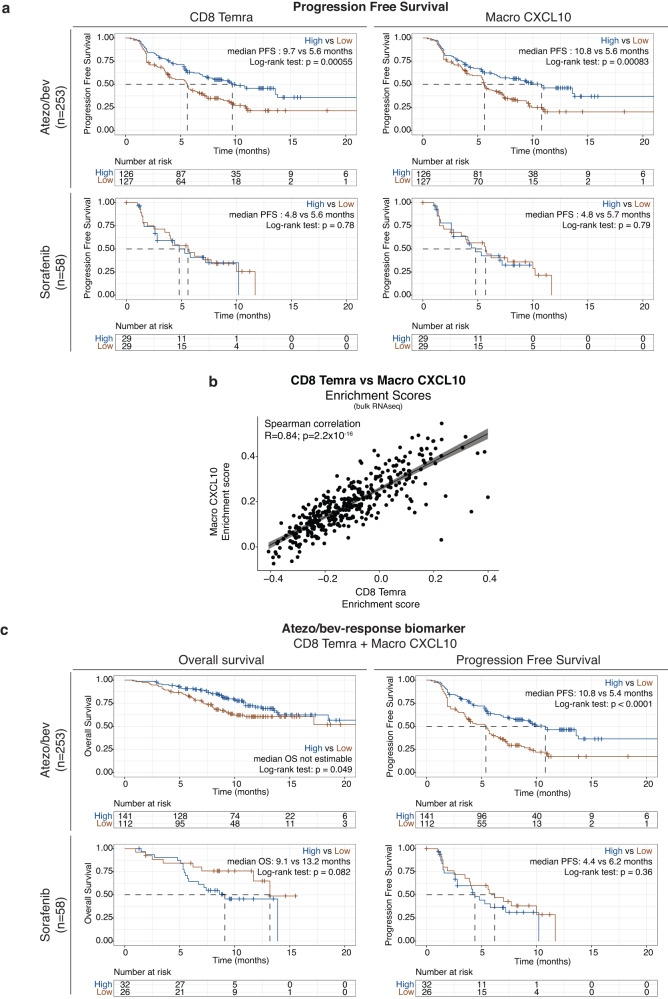
The combination of atezolizumab plus bevacizumab (atezo/bev) has dramatically changed the treatment landscape of advanced HCC (aHCC), achieving durable responses in some patients. Using single-cell transcriptomics, we characterize the intra-tumoural and peripheral immune context of patients with aHCC treated with atezo/bev. Tumours from patients with durable responses are enriched for PDL1+ CXCL10+ macrophages and, based on cell-cell interaction analysis, express high levels of CXCL9/10/11 and are predicted to attract peripheral CXCR3+ CD8+ effector-memory T cells (CD8 TEM) into the tumour. Based on T cell receptor sharing and pseudotime trajectory analysis, we propose that CD8 TEM preferentially differentiate into clonally-expanded PD1- CD45RA+ effector-memory CD8+ T cells (CD8 TEMRA) with pronounced cytotoxicity. In contrast, in non-responders, CD8 TEM remain frozen in their effector-memory state. Finally, in responders, CD8 TEMRA display a high degree of T cell receptor sharing with blood, consistent with their patrolling activity. These findings may help understand the possible mechanisms underlying response to atezo/bev in aHCC.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
- 1S95221N/Fonds Wetenschappelijk Onderzoek (Research Foundation Flanders)
- FAF-C/2018/1297/Stichting Tegen Kanker (Belgian Foundation Against Cancer)
- Advanced grant 101055422/EC | EU Framework Programme for Research and Innovation H2020 | H2020 Priority Excellent Science | H2020 European Research Council (H2020 Excellent Science - European Research Council)
- Internal fund C14/18/092/KU Leuven (Katholieke Universiteit Leuven)
LinkOut - more resources
Full Text Sources
Medical
Research Materials
