

Sex Differences in the Clinical Presentation and Natural History of Dilated Cardiomyopathy
- PMID: 38032570
- PMCID: PMC10857810
- DOI: 10.1016/j.jchf.2023.10.009
Sex Differences in the Clinical Presentation and Natural History of Dilated Cardiomyopathy
Abstract
Background: Biological sex has a diverse impact on the cardiovascular system. Its influence on dilated cardiomyopathy (DCM) remains unresolved.
Objectives: This study aims to investigate sex-specific differences in DCM presentation, natural history, and prognostic factors.
Methods: The authors conducted a prospective observational cohort study of DCM patients assessing baseline characteristics, cardiac magnetic resonance imaging, biomarkers, and genotype. The composite outcome was cardiovascular mortality or major heart failure (HF) events.
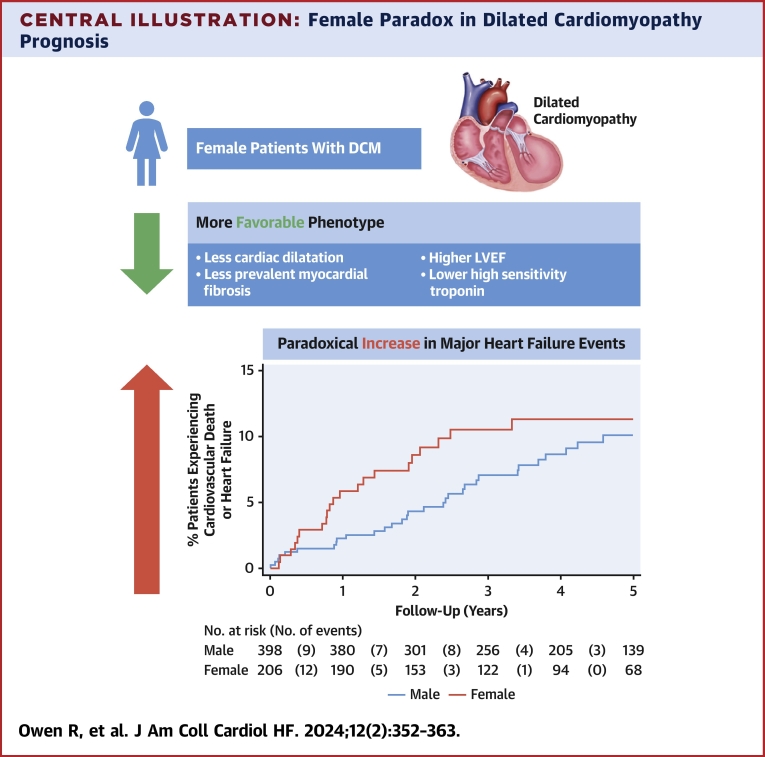
Results: Overall, 206 females and 398 males with DCM were followed for a median of 3.9 years. At baseline, female patients had higher left ventricular ejection fraction, smaller left ventricular volumes, less prevalent mid-wall myocardial fibrosis (23% vs 42%), and lower high-sensitivity cardiac troponin I than males (all P < 0.05) with no difference in time from diagnosis, age at enrollment, N-terminal pro-B-type natriuretic peptide levels, pathogenic DCM genetic variants, myocardial fibrosis extent, or medications used for HF. Despite a more favorable profile, the risk of the primary outcome at 2 years was higher in females than males (8.6% vs 4.4%, adjusted HR: 3.14; 95% CI: 1.55-6.35; P = 0.001). Between 2 and 5 years, the effect of sex as a prognostic modifier attenuated. Age, mid-wall myocardial fibrosis, left ventricular ejection fraction, left atrial volume, N-terminal pro-B-type natriuretic peptide, high-sensitivity cardiac troponin I, left bundle branch block, and NYHA functional class were not sex-specific prognostic factors.
Conclusions: The authors identified a novel paradox in prognosis for females with DCM. Female DCM patients have a paradoxical early increase in major HF events despite less prevalent myocardial fibrosis and a milder phenotype at presentation. Future studies should interrogate the mechanistic basis for these sex differences.
Keywords: females; heart; males; sex.
Crown Copyright © 2024. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This work was supported by the UK Medical Research Council (MR/W023830/1), the National Heart Lung Institute Research Foundation, Royston Centre for Cardiomyopathy Research, NIHR Biomedical Research Unit Royal Brompton Hospital, NIHR Imperial College Biomedical Research Centre, British Heart Foundation (RE/18/4/34215; SP/10/10/28431; SP/17/11/32885; BH FS/ICRF/21/26019), Wellcome Trust (107469/Z/15/Z), Rosetrees Trust, Sir Jules Thorn Charitable Trust [21JTA], and Alexander Jansons Myocarditis UK. Dr Januzzi has been supported in part by the Hutter Family Professorship. Dr Van Spall has been funded by the Canadian Institutes of Health Research and Heart and Stroke Foundation of Canada. Dr Michos has participated in advisory boards for Novo Nordisk, Novartis, Bayer, Esperion, AstraZeneca, and Amarin. Dr Januzzi has been a trustee of the American College of Cardiology; has been a board member of Imbria Pharmaceuticals; has been a director at Jana Care; has received grant support from Abbott Diagnostics, Applied Therapeutics, HeartFlow, Innolife, and LivaNova; has received consulting fees from Abbott, Bayer, Beckman-Coulter, Boehringer-Ingelheim, Janssen, Novartis, Quidel, Roche Diagnostics, and Siemens; and has participated in clinical endpoint committees/data safety monitoring boards for Abbott, AbbVie, Bayer, CVRx, Intercept, Pfizer, and Takeda. Dr Pennell has received consulting fees from Bayer and Chiesi; has received research support from Bayer and Siemens; and has received speaker fees from Chiesi and Bayer. Dr Cook has been a co-founder and shareholder with Enleofen Bio PTE LTD. Dr Ware has received consulting fees from MyoKardia and Foresite Labs; and has received research support from MyoKardia/Bristol Myers Squibb. Dr Halliday has participated in an advisory board with AstraZeneca. Dr Baruah is working full-time for AstraZeneca. For the purpose of open access, the author has applied a Creative Commons Attribution (CC BY) licence to any Author Accepted Manuscript version arising. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures





Comment in
-
Dilated Cardiomyopathy Presentation, Early Outcomes, and Female Sex: A Paradox Revealed.JACC Heart Fail. 2024 Feb;12(2):364-365. doi: 10.1016/j.jchf.2023.11.013. JACC Heart Fail. 2024. PMID: 38326001 No abstract available.
References
-
- Gulati A., Jabbour A., Ismail T.F., et al. Association of fibrosis with mortality and sudden cardiac death in patients with nonischemic dilated cardiomyopathy. JAMA. 2013;309:896–908. - PubMed
-
- Vogel B., Acevedo M., Appelman Y., et al. The Lancet Women and Cardiovascular Disease Commission: reducing the global burden by 2030. Lancet. 2021;397:2385–2438. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
