

Monocyte to Lymphocyte ratio is highly specific in diagnosing latent tuberculosis and declines significantly following tuberculosis preventive therapy: A cross-sectional and nested prospective observational study
- PMID: 38033005
- PMCID: PMC10688757
- DOI: 10.1371/journal.pone.0291834
Monocyte to Lymphocyte ratio is highly specific in diagnosing latent tuberculosis and declines significantly following tuberculosis preventive therapy: A cross-sectional and nested prospective observational study
Abstract
Background: Interferon-gamma release assay and tuberculin skin test use is limited by costly sundries and cross-reactivity with non-tuberculous mycobacteria and Bacille Calmette-Guérin (BCG) vaccination respectively. We investigated the Monocyte to Lymphocyte ratio (MLR) as a biomarker to overcome these limitations and for use in monitoring response to tuberculosis preventive therapy (TPT).
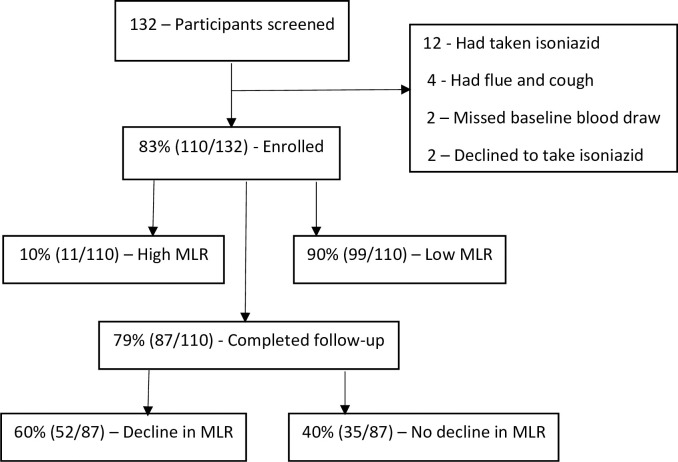
Methods: We conducted a cross-sectional and nested prospective observational study among asymptomatic adults living with Human Immuno-deficiency Virus (HIV) in Kampala, Uganda. Complete blood count (CBC) and QuantiFERON-TB® Gold-plus were measured at baseline and CBC repeated at three months. Multivariable logistic regression was performed to identify factors associated with a high MLR and decline in MLR.
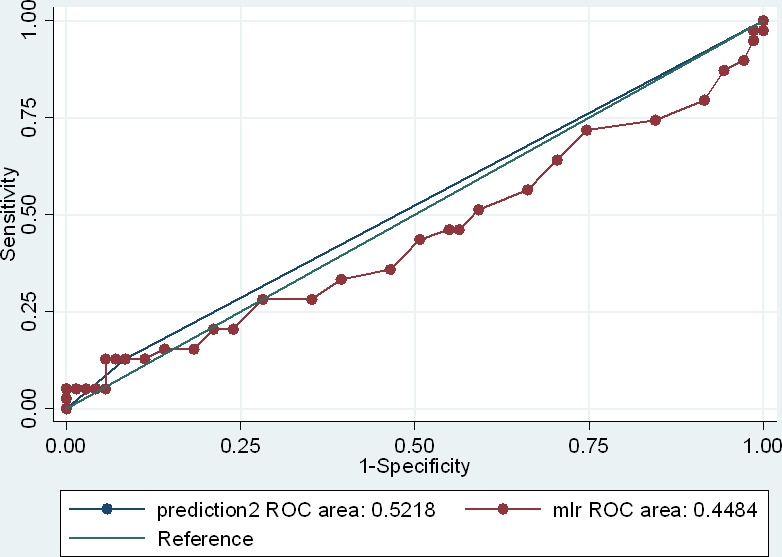
Results: We recruited 110 adults living with HIV and on antiretroviral therapy, of which 82.5% (85/110) had suppressed viral loads, 71.8% (79/110) were female, and 73.6% (81/110) had a BCG scar. The derived MLR diagnostic cut-off was 0.35, based on which the MLR sensitivity, specificity, positive predictive value, and negative predictive value were 12.8%, 91.6%, 45.5%, and 65.7% respectively. The average MLR declined from 0.212 (95% CI: 0.190-0.235) at baseline to 0.182 (95% CI: 0.166-0.198) after three months of TPT. A viral load of >50 copies/ml (aOR, 5.67 [1.12-28.60]) was associated with a high MLR while that of <50 copies/ml (aOR, 0.07 [0.007-0.832]) was associated with a decline in MLR.
Conclusion: MLR was highly specific in diagnosing latent TB and declined significantly following three months of TPT. Implications of a high MLR and decline in MLR after TPT need further evaluation in a larger cohort.
Copyright: © 2023 Mayito et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- WHO. The END TB Strategy. [Internet]. 2015. Aug.
-
- World Health Organization (2011). Use of Tuberculosis Interferon-Gamma Release Assays (IGRAs) in Low- and Middle- Income Countries: Policy Statement. [Internet]. 2011. - PubMed
-
- WHO. WHO TB KNOWLEDGE SHARING PLATFORM: WHO-recommended four-symptom screen. [Internet]. 2021.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
