

The epidemiology of superficial Streptococcal A (impetigo and pharyngitis) infections in Australia: A systematic review
- PMID: 38033025
- PMCID: PMC10688633
- DOI: 10.1371/journal.pone.0288016
The epidemiology of superficial Streptococcal A (impetigo and pharyngitis) infections in Australia: A systematic review
Abstract
Background: Streptoccocal A (Strep A, GAS) infections in Australia are responsible for significant morbidity and mortality through both invasive (iGAS) and post-streptococcal (postGAS) diseases as well as preceding superficial (sGAS) skin and throat infection. The burden of iGAS and postGAS are addressed in some jurisdictions by mandatory notification systems; in contrast, the burden of preceding sGAS has no reporting structure, and is less well defined. This review provides valuable, contemporaneous evidence on the epidemiology of sGAS presentations in Australia, informing preventative health projects such as a Streptococcal A vaccine and standardisation of primary care notification.
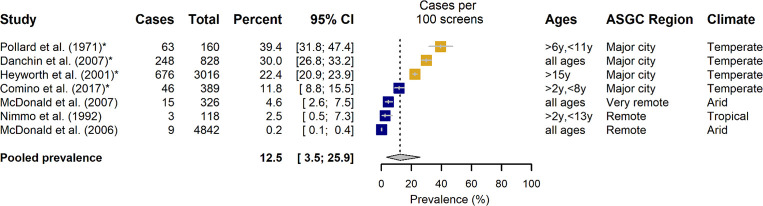
Methods and findings: MEDLINE, Scopus, EMBASE, Web of Science, Global Health, Cochrane, CINAHL databases and the grey literature were searched for studies from an Australian setting relating to the epidemiology of sGAS infections between 1970 and 2020 inclusive. Extracted data were pooled for relevant population and subgroup analysis. From 5157 titles in the databases combined with 186 grey literature reports and following removal of duplicates, 4889 articles underwent preliminary title screening. The abstract of 519 articles were reviewed with 162 articles identified for full text review, and 38 articles identified for inclusion. The majority of data was collected for impetigo in Aboriginal and Torres Strait Islander populations, remote communities, and in the Northern Territory, Australia. A paucity of data was noted for Aboriginal and Torres Strait Islander people living in urban centres or with pharyngitis. Prevalence estimates have not significantly changed over time. Community estimates of impetigo point prevalence ranged from 5.5-66.1%, with a pooled prevalence of 27.9% [95% CI: 20.0-36.5%]. All studies excepting one included >80% Aboriginal and Torres Strait Islander people and all excepting two were in remote or very remote settings. Observed prevalence of impetigo as diagnosed in healthcare encounters was lower, with a pooled estimate of 10.6% [95% CI: 3.1-21.8%], and a range of 0.1-50.0%. Community prevalence estimates for pharyngitis ranged from 0.2-39.4%, with a pooled estimate of 12.5% [95% CI: 3.5-25.9%], higher than the prevalence of pharyngitis in healthcare encounters; ranging from 1.0-5.0%, and a pooled estimate of 2.0% [95% CI: 1.3-2.8%]. The review was limited by heterogeneity in study design and lack of comparator studies for some populations.
Conclusions: Superficial Streptococcal A infections contribute to an inequitable burden of disease in Australia and persists despite public health interventions. The burden in community studies is generally higher than in health-services settings, suggesting under-recognition, possible normalisation and missed opportunities for treatment to prevent postGAS. The available, reported epidemiology is heterogeneous. Standardised nation-wide notification for sGAS disease surveillance must be considered in combination with the development of a Communicable Diseases Network of Australia (CDNA) Series of National Guideline (SoNG), to accurately define and address disease burden across populations in Australia.
Trial registration: This review is registered with PROSPERO. Registration number: CRD42019140440.
Copyright: © 2023 Wiegele et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures






Update of
-
Protocol for the systematic review of the epidemiology of superficial Streptococcal A infections (skin and throat) in Australia.PLoS One. 2021 Aug 11;16(8):e0255789. doi: 10.1371/journal.pone.0255789. eCollection 2021. PLoS One. 2021. Update in: PLoS One. 2023 Nov 30;18(11):e0288016. doi: 10.1371/journal.pone.0288016. PMID: 34379660 Free PMC article. Updated.
References
-
- Ralph A, Carapetis J. Group A Streptococcal Diseases and Their Global Burden Host-Pathogen Interactions in Streptococcal Diseases. Curr Top Microbiol. 2013;368:1–27. - PubMed
-
- Wright CM, Langworthy K, Manning L. The Australian burden of invasive group A streptococcal disease–a narrative review. Intern Med J. 2020;51(6). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
