

Avoiding Surgery: Endoscopic Treatment of Congenital Duodenal Stenosis
- PMID: 38034463
- PMCID: PMC10684216
- DOI: 10.1097/PG9.0000000000000347
Avoiding Surgery: Endoscopic Treatment of Congenital Duodenal Stenosis
Abstract
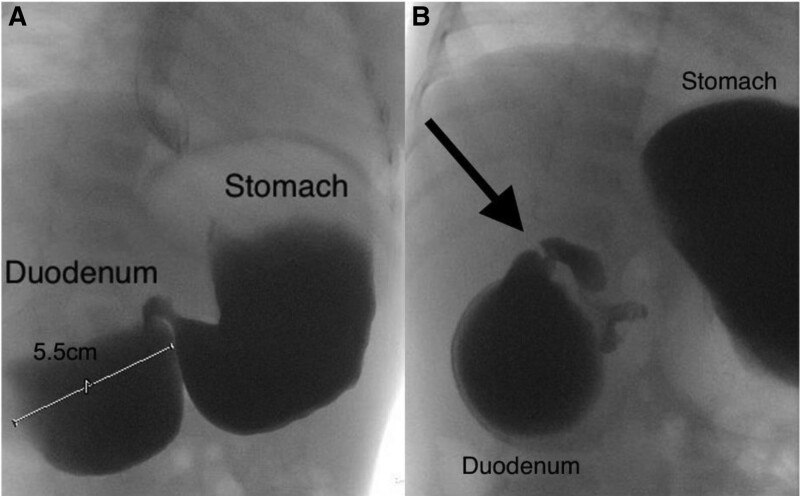
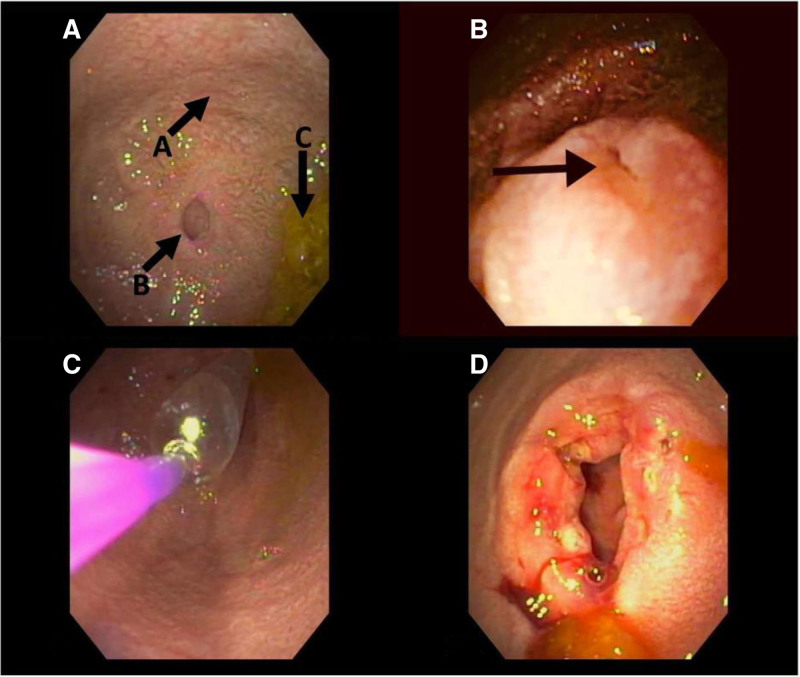
Duodenal stenosis is a rare congenital anomaly that is typically treated surgically, although endoscopic incisional therapy (EIT) and balloon dilation are minimally invasive alternatives. We present a case of a 15-month-old male with vomiting and difficulty tolerating solid food due to severe congenital duodenal stenosis. The patient underwent EIT and serial duodenal dilation to a diameter of 20 mm, which resulted in significant symptom improvement. Intralesional corticosteroid injection (ISI) was administered to help prevent the duodenal septum from restricturing. The combination of EIT, balloon dilation, and ISI was successful in treating the patient's congenital duodenal stenosis and avoided the need for surgery. However, further studies are required to confirm the efficacy of this treatment approach in this patient population. This report highlights the potential of this minimally invasive approach as an alternative to surgical intervention in the management of congenital duodenal stenosis.
Keywords: endoscopic balloon dilation; endoscopy; intralesional corticosteroid injection; membranous duodenal web; radial incisional therapy.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Williams SA, Nguyen ATH, Chang H, et al. . Multicenter comparison of laparoscopic versus open repair of duodenal atresia in neonates. J Laparoendosc Adv Surg Tech A. 2022;32:226–230. - PubMed
-
- Huang MH, Bian HQ, Liang C, et al. . Gastroscopic treatment of membranous duodenal stenosis in infants and children: report of 6 cases. J Pediatr Surg. 2015;50:413–416. - PubMed
-
- Beeks A, Gosche J, Giles H, et al. . Endoscopic dilation and partial resection of a duodenal web in an infant. J Pediatr Gastroenterol Nutr. 2009;48:378–381. - PubMed
-
- Muensterer OJ, Hansen EN. Resection of a duodenal web using single-incision pediatric endosurgery. J Pediatr Surg. 2011;46:989–993. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
