Clostridioides difficile infection leading to fulminant colitis with toxic megacolon
- PMID: 38034515
- PMCID: PMC10687841
- DOI: 10.4322/acr.2023.457
Clostridioides difficile infection leading to fulminant colitis with toxic megacolon
Abstract
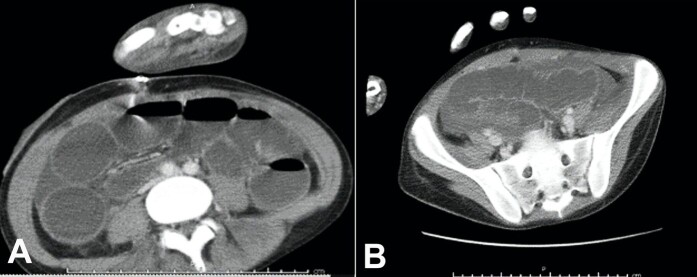
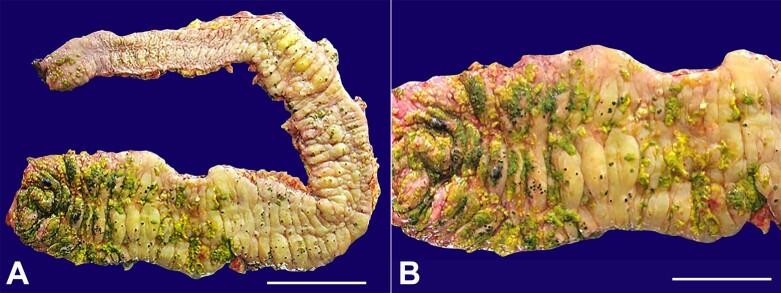
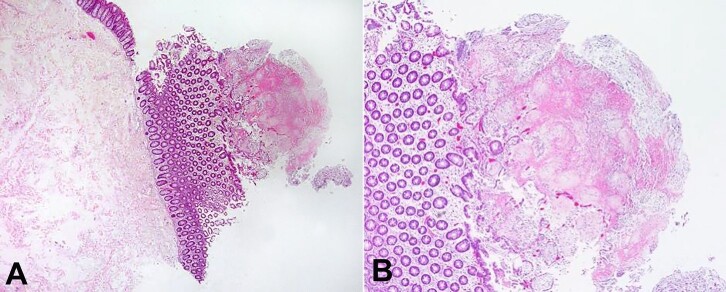
Clostridioidesdifficile infection (CDI) is the culprit of millions of nosocomial infections in the United States. Programs that successfully decrease its incidence, therefore, render cost savings for the healthcare system. Toxic megacolon and perforation are two of the most significant complications with increased mortality rates. We report a 23-year-old nursing home resident hospitalized for fever, cough, and green sputum. After 3 days of antibiotic therapy, he developed abdominal distension, diarrhea, and vomiting and underwent a total colectomy. The colon was dilated to a maximum of 11 cm with markedly edematous mucosa and yellow pseudomembranes. Qualitative PCR of the stool detected Clostridioides difficile toxin B gene. While there is no consensus for the required interval between antibiotic treatment and CDI, this presentation 3 days after starting the antibiotic therapy is earlier than most proposed ranges.
Keywords: Colectomy; Colitis; Colorectal Surgery; Diarrhea, Pseudomembranous.
Copyright © 2023 The Authors.
Conflict of interest statement
Conflict of interest: None
Figures