Radiologic-pathologic autopsy correlation of an internal watershed infarct, a case report
- PMID: 38034516
- PMCID: PMC10687791
- DOI: 10.4322/acr.2023.448
Radiologic-pathologic autopsy correlation of an internal watershed infarct, a case report
Abstract
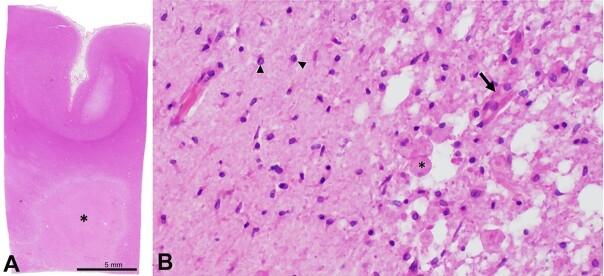
Internal watershed infarcts (IWIs) occur at the junction of the deep and superficial perforating arterial branches of the cerebrum. Despite documentation in the radiology literature, IWIs are rarely encountered at the time of autopsy. Here, we report the case of a 59-year-old incarcerated male who was brought to the emergency department after being found unresponsive on the floor of his jail cell. Initial examination and imaging demonstrated right-sided hemiplegia, aphasia, right facial droop, and severe stenosis of the left middle cerebral artery, respectively. Repeat imaging 4 days after admission and 26 days before death demonstrated advanced stenosis of the intracranial, communicating segment of the right internal carotid artery, a large acute infarct in the right posterior cerebral artery territory, and bilateral deep white matter ischemic changes with a right-sided "rosary-like" pattern of injury that is typical of IWIs. Postmortem gross examination showed that the right deep white matter lesion had progressed to a confluent, "cigar-shaped" subacute IWI involving the right corona radiata. This is the first well-documented case of an IWI with radiologic imaging and photographic gross pathology correlation. This case uniquely highlights a rarely encountered lesion at the time of autopsy and provides an excellent visual representation of internal watershed neuroanatomy.
Keywords: Internal watershed; autopsy; infarction; neuropathology.
Copyright: © 2023 The Authors.
Conflict of interest statement
Conflict of interest: None.
Figures