

A retrospective study of laparoscopic, robotic-assisted, and open emergent/urgent cholecystectomy based on the PINC AI Healthcare Database 2017-2020
- PMID: 38037087
- PMCID: PMC10687827
- DOI: 10.1186/s13017-023-00521-8
A retrospective study of laparoscopic, robotic-assisted, and open emergent/urgent cholecystectomy based on the PINC AI Healthcare Database 2017-2020
Abstract
Background: Robotic-assisted cholecystectomy (RAC) is becoming increasingly common, but the outcomes of emergent/urgent robotic-assisted cholecystectomies compared to emergent laparoscopic (LC) and open cholecystectomies (OC) remain understudied.
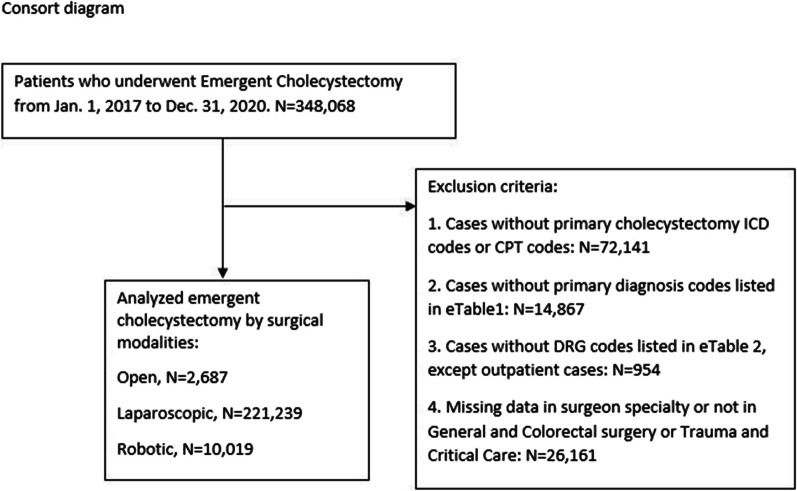
Methods: The PINC AI Healthcare Database was queried to identify adults who underwent emergent or urgent (Em-Ur) cholecystectomy between January 1, 2017, and December 31, 2020. Immediate postoperative and 30-day outcomes were identified including intraoperative complications, transfusion, conversion, postoperative complication, and hospital length of stay. Propensity score matching was done to compare outcomes between Em-Ur robotic-assisted, laparoscopic, and open cholecystectomies Subgroup analyses were performed comparing RAC done with and without fluorescent imaging as well as comparing RAC and LC performed for patients with class 3 obesity (BMI ≥ 40 kg/m2).
Results: RAC Em-Ur cholecystectomies are being performed with increasing frequency and is the most utilized modality for patients with class 3 obesity. There was no difference in intraoperative complications (0.3%), bile duct injury (0.2%), or postoperative outcomes between RAC and LC. LC had significantly shorter operating room times (96 min (75,128)) compared to RAC (120 min (90,150)). There was a significant lower rate of conversion to open in RAC (1.9%) relative to LC (3.2%) in both the overall population and the class 3 obesity sub-analysis (RAC-2.6% vs. LC-4.4%). There was no difference in outcomes in robotic-assisted cholecystectomies done with and without fluorescent imaging.
Conclusions: A comparison of propensity score-matched cohorts of emergent/urgent robotic-assisted and laparoscopic cholecystectomy indicates that robotic-assisted cholecystectomy is a safe alternative to laparoscopic cholecystectomy, and that both have superior outcomes to open cholecystectomies.
© 2023. The Author(s).
Conflict of interest statement
SC—no disclosures; SHL—employed by Intuitive Surgical; YL—employed by Intuitive Surgical; and SMW—consultant to Intuitive Surgical.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
