

An Italian case series' description of thiamine responsive megaloblastic anemia syndrome: importance of early diagnosis and treatment
- PMID: 38037112
- PMCID: PMC10691017
- DOI: 10.1186/s13052-023-01553-1
An Italian case series' description of thiamine responsive megaloblastic anemia syndrome: importance of early diagnosis and treatment
Abstract
Background: Individuals with thiamine-responsive megaloblastic anemia (TRMA) mainly manifest macrocytic anemia, sensorineural deafness, ocular complications, and nonautoimmune diabetes. Macrocytic anemia and diabetes may be responsive to high-dosage thiamine treatment, in contrast to sensorineural deafness. Little is known about the efficacy of thiamine treatment on ocular manifestations.
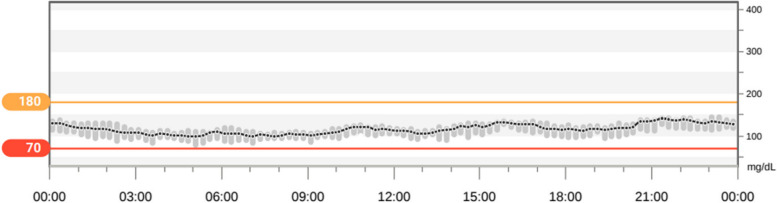
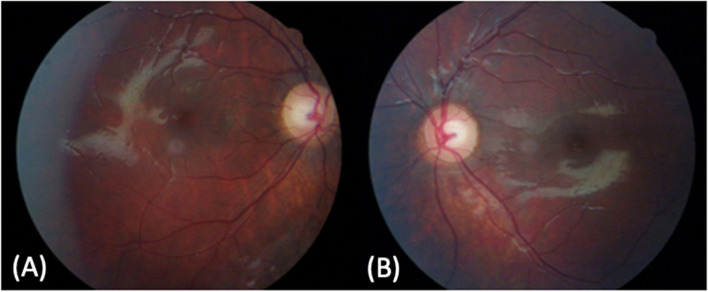
Cases presentation: Our objective is to report data from four Italian TRMA patients: in Cases 1, 2 and 3, the diagnosis of TRMA was made at 9, 14 and 27 months. In 3 out of 4 subjects, thiamine therapy allowed both normalization of hyperglycemia, with consequent insulin suspension, and macrocytic anemia. In all Cases, thiamine therapy did not resolve the clinical manifestation of deafness. In Cases 2 and 3, follow-up showed no blindness, unlike Case 4, in which treatment was started for megaloblastic anemia at age 7 but was increased to high doses only at age 25, when the genetic diagnosis of TRMA was performed.
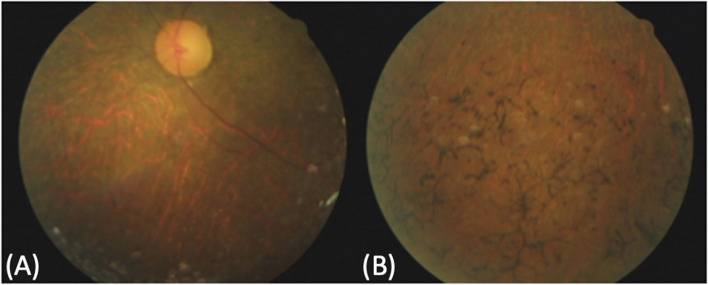
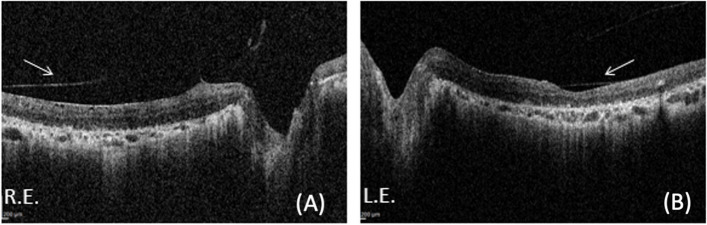
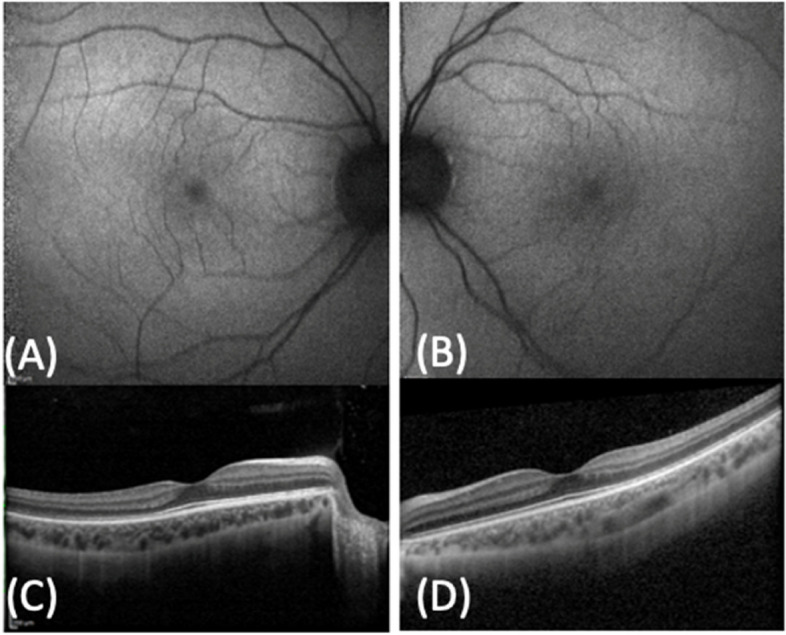
Conclusions: Early institution of high-dose thiamine supplementation seems to prevent the development of retinal changes and optic atrophy in TRMA patients. The spectrum of clinical manifestations is broad, and it is important to describe known Cases to gain a better understanding of this rare disease.
Keywords: Case series; Nonautoimmune diabetes; Optic atrophy; Sensorineural deafness; Thiamine-responsive megaloblastic anemia syndrome.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Thiamine responsive megaloblastic anemia: a novel SLC19A2 compound heterozygous mutation in two siblings.Pediatr Diabetes. 2013 Aug;14(5):384-7. doi: 10.1111/j.1399-5448.2012.00921.x. Epub 2013 Jan 4. Pediatr Diabetes. 2013. PMID: 23289844
-
An Adult Case of Thiamine-Sensitive Megaloblastic Anemia Syndrome Accidentally Diagnosed Myelodysplastic Syndrome.J Coll Physicians Surg Pak. 2019 Jun;29(6):S13-S15. doi: 10.29271/jcpsp.2019.06.S13. J Coll Physicians Surg Pak. 2019. PMID: 31142407
-
Leber congenital amaurosis as an initial manifestation in a Chinese patient with thiamine-responsive megaloblastic anemia syndrome.Am J Med Genet A. 2022 Mar;188(3):948-952. doi: 10.1002/ajmg.a.62582. Epub 2021 Nov 25. Am J Med Genet A. 2022. PMID: 34821467
-
[Thiamine-responsive megaloblastic anemia or Rogers syndrome: A literature review].Rev Med Interne. 2019 Jan;40(1):20-27. doi: 10.1016/j.revmed.2018.06.005. Epub 2018 Jul 19. Rev Med Interne. 2019. PMID: 30031565 Review. French.
-
Long-term follow-up of diabetes in two patients with thiamine-responsive megaloblastic anemia syndrome.Diabetes Care. 1998 Jan;21(1):38-41. doi: 10.2337/diacare.21.1.38. Diabetes Care. 1998. PMID: 9538968 Review.
Cited by
-
The association between anemia and sensorineural hearing loss: A review.Medicine (Baltimore). 2024 Nov 1;103(44):e40326. doi: 10.1097/MD.0000000000040326. Medicine (Baltimore). 2024. PMID: 39496053 Free PMC article. Review.
-
Diagnosis of a patient with severe sensorineural hearing loss as the initial symptom caused by novel compound heterozygous variant in SLC19A2 gene.Braz J Otorhinolaryngol. 2025 Jul-Aug;91(4):101581. doi: 10.1016/j.bjorl.2025.101581. Epub 2025 Apr 11. Braz J Otorhinolaryngol. 2025. PMID: 40220483 Free PMC article.
-
Neonatal and Syndromic Forms of Diabetes.Curr Diab Rep. 2025 Mar 25;25(1):26. doi: 10.1007/s11892-024-01567-x. Curr Diab Rep. 2025. PMID: 40128490 Free PMC article. Review.
References
-
- Raz T, Labay V, Baron D, Szargel R, Anbinder Y, Barrett T, Rabl W, Viana MB, Mandel H, Baruchel A, Cayuela JM, Cohen N. The spectrum of mutations, including four novel ones, in the thiamine-responsive megaloblastic anemia gene SLC19A2 of eight families T. Hum Mutat. 2000;16(1):37–42. doi: 10.1002/1098-1004. - DOI - PubMed
-
- Franzese A, Fattorusso V, Mozzillo E. Thiamine-responsive megaloblastic anemia syndrome” in diabetes associated with single gene defects and chromosomal abnormalities. Front Diabetes Basel Karger. 2017;25:49–54. doi: 10.1159/000454700. - DOI
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
