

Altered Bile Acid and Pouch Microbiota Composition in Patients With Chronic Pouchitis
- PMID: 38037191
- PMCID: PMC11219471
- DOI: 10.1093/ibd/izad288
Altered Bile Acid and Pouch Microbiota Composition in Patients With Chronic Pouchitis
Abstract
Background: Patients with ulcerative colitis and total abdominal proctocolectomy with ileal pouch-anal anastomosis have a 50% risk of pouchitis and a 5% to 10% risk of chronic pouchitis.
Aims: The goal of the study was to compare pouch microbiota and stool bile acid composition in patients with chronic pouchitis, chronic pouchitis and primary sclerosing cholangitis, and normal pouch.
Methods: Patients with ulcerative colitis and ileal pouch-anal anastomosis were recruited from March 20, 2014, to August 6, 2019, and categorized into normal pouch, chronic pouchitis, and chronic pouchitis/primary sclerosing cholangitis groups. Stool samples were subjected to bile acid quantification and 16S rRNA gene sequencing. Statistical comparisons of absolute bile acid abundance and pouch microbiota α-diversity, β-diversity, and taxa abundance were performed among the patient groups.
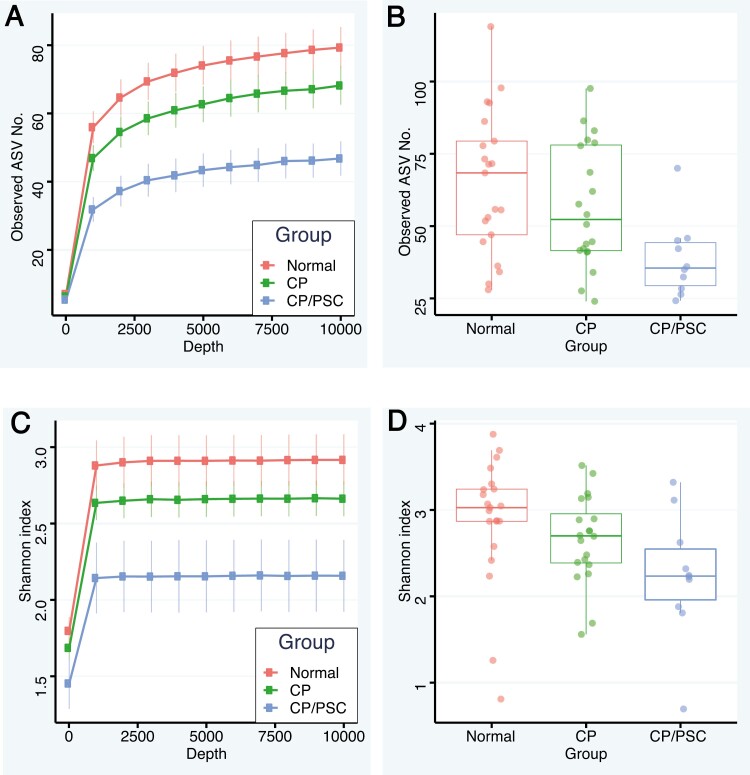
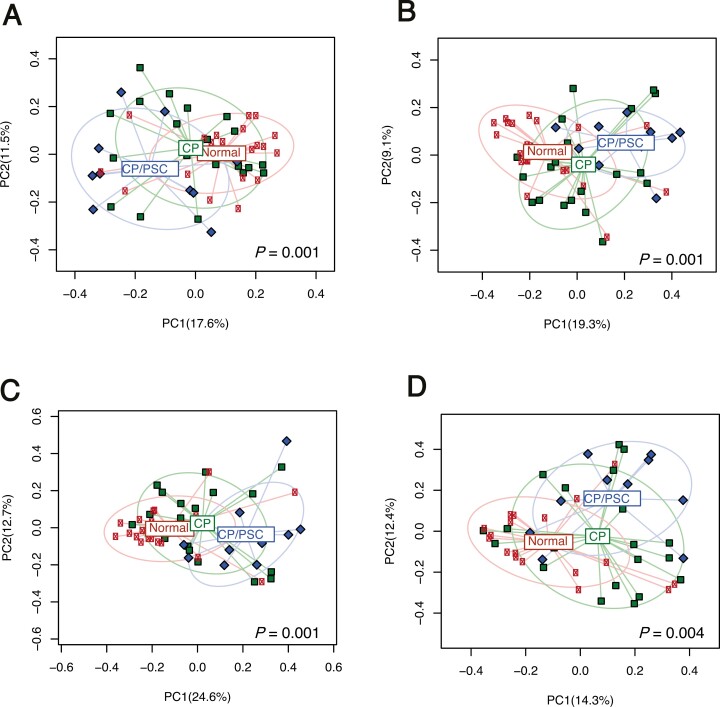
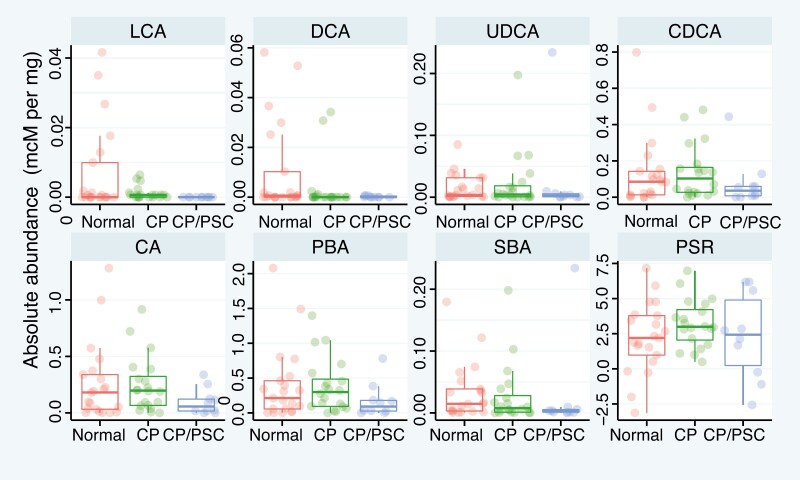
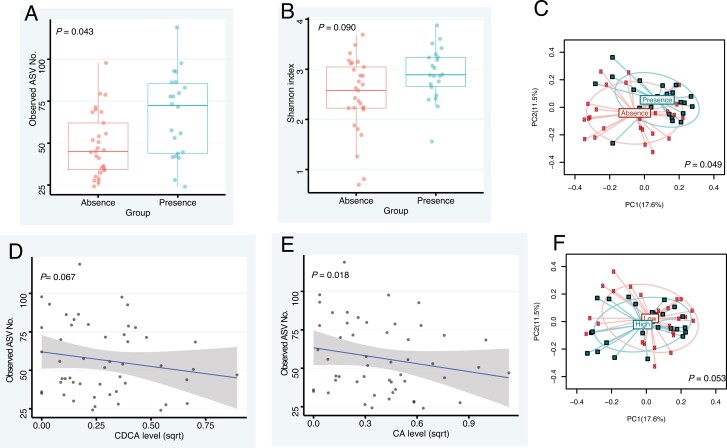
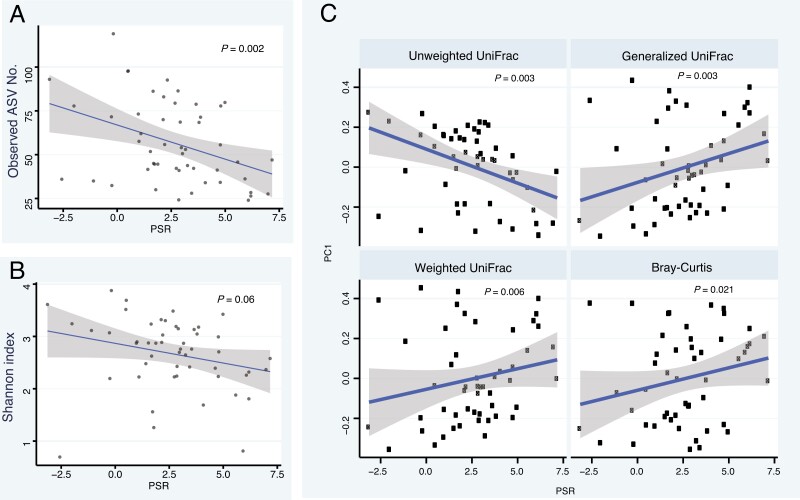
Results: A total of 51 samples were analyzed. Both α-diversity (P = .01, species richness) and β-diversity (P = .001) significantly differed among groups. Lithocholic acid was significantly lower in patients with chronic pouchitis/primary sclerosing cholangitis than in those with chronic pouchitis (P = .01) or normal pouch (P = .03). Decreased α-diversity was associated with an increased primary to secondary bile acid ratio (P = .002), which was also associated with changes in β-diversity (P = .006).
Conclusions: Pouch microbiota α- and β-diversity differed among patients with normal pouch, chronic pouchitis, and chronic pouchitis/primary sclerosing cholangitis. Lithocholic acid level and primary to secondary bile acid ratio were highly associated with pouch microbiota richness, structure, and composition. These findings emphasize the associations between pouch microbiota and bile acid composition in dysbiosis and altered metabolism, suggesting that secondary bile acids are decreased in chronic pouchitis.
Keywords: inflammatory bowel disease; microbiome; pouchitis; primary sclerosing cholangitis; ulcerative colitis.
Plain language summary
The α- and β-diversity of the pouch microbiota significantly differed in chronic pouchitis, chronic pouchitis and primary sclerosing cholangitis, and normal pouch. Microbiota changes were associated with stool bile acid composition. Decreased diversity was associated with decreased secondary bile acids.
© The Author(s) 2023. Published by Oxford University Press on behalf of Crohn’s & Colitis Foundation. All rights reserved. For commercial re-use, please contact reprints@oup.com for reprints and translation rights for reprints. All other permissions can be obtained through our RightsLink service via the Permissions link on the article page on our site—for further information please contact journals.permissions@oup.com.
Conflict of interest statement
L.R., Janssen Pharmaceuticals—Advisory board
Figures
Comment in
-
Altered Bile Acids and Pouch Microbiota Composition in Patients With Chronic Pouchitis.Inflamm Bowel Dis. 2025 Apr 10;31(4):1184-1187. doi: 10.1093/ibd/izaf005. Inflamm Bowel Dis. 2025. PMID: 40073325
References
-
- Quinn KP, Lightner AL, Faubion WA, Raffals LE.. A comprehensive approach to pouch disorders. Inflamm Bowel Dis. 2019;25(3):460-471. - PubMed
-
- Quinn KP, Urquhart SA, Janssens LP, et al.Primary sclerosing cholangitis-associated pouchitis: a distinct clinical phenotype. Clin Gastroenterol Hepatol. 2022;20(5):e964-e973. - PubMed
-
- Shen B. Acute and chronic pouchitis--pathogenesis, diagnosis and treatment. Nat Rev Gastroenterol Hepatol. 2012;9(6):323-333. - PubMed
-
- Reshef L, Kovacs A, Ofer A, et al.Pouch inflammation is associated with a decrease in specific bacterial taxa. Gastroenterology. 2015;149(3):718-727. - PubMed
-
- Dubinsky V, Reshef L, Bar N, et al.Predominantly antibiotic-resistant intestinal microbiome persists in patients with pouchitis who respond to antibiotic therapy. Gastroenterology. 2020;158(3):610-624.e13. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
