

CT and 18FDG-PET/CT findings in progressive mediastinal idiopathic fibrosis as a benign mimicker of esophageal carcinoma: a case report
- PMID: 38041832
- PMCID: PMC10693803
- DOI: 10.1177/03000605231213212
CT and 18FDG-PET/CT findings in progressive mediastinal idiopathic fibrosis as a benign mimicker of esophageal carcinoma: a case report
Abstract
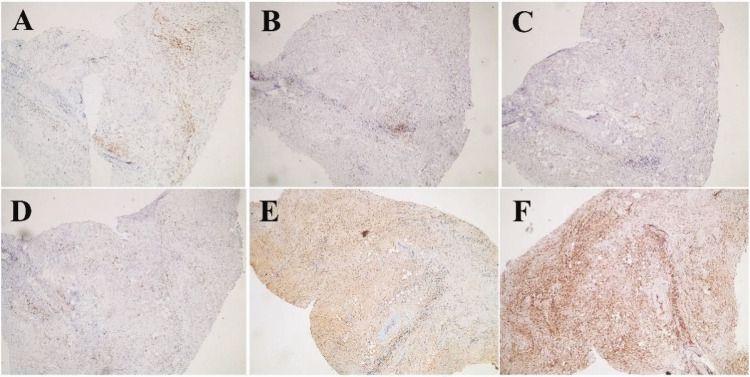
Idiopathic mediastinal fibrosis, also called sclerosing or fibrosing mediastinitis, is a very rare and aggressive fibroinflammatory process characterized by fibrous tissue proliferation in the mediastinal region. Herein, we present a rare case of idiopathic mediastinal fibrosis presenting with esophageal obstruction, most likely associated with immunoglobulin G (IgG4)-related disease, affecting the posterior mediastinum with intrapulmonary infiltration. Computed tomography revealed a narrowed lumen and thickened wall of the distal esophagus surrounded by a necrotic mass with infiltration into the nearby structures, suggesting a locally advanced malignant process. Positron emission tomography revealed intense accumulation of 18F-fluorodeoxyglucose, indicating an active inflammatory component, which complicates further differential diagnosis of mediastinal masses. Thoracoscopic biopsy and immunohistochemical analysis confirmed a fibroinflammatory process with perivascular lymphoid cell infiltration that was cluster of differentiation (CD)3 (++) and CD20 (++), with massive numbers of IgG4-immunoreactive plasma cells. Although a benign condition, sclerosing mediastinitis is a close mimicker of esophageal carcinoma, which cannot be differentiated by computed tomography or positron emission tomography and must be considered in a differential diagnosis.
Keywords: Idiopathic mediastinal fibrosis; IgG4-related disease; case report; computed tomography; differential diagnosis; esophageal carcinoma; positron emission tomography.
Conflict of interest statement
Declaration of conflicting interestsThe authors declare that there is no conflict of interest.
Figures




References
-
- Rossi GM, Emmi G, Corradi D, et al.. Idiopathic mediastinal fibrosis: a systemic immune-mediated disorder. A case series and a review of the literature. Clin Rev Allergy Immunol 2017; 52: 446–459. - PubMed
-
- Hanley PC, Shub C, Lie JT. Constrictive pericarditis associated with combined idiopathic retroperitoneal and mediastinal fibrosis. Mayo Clin Proc 1984; 59: 300–304. - PubMed
-
- Dechambre S, Dorzee J, Fastrez J, et al.. Bronchial stenosis and sclerosing mediastinitis: an uncommon complication of external thoracic radiotherapy. Eur Respir J 1998; 11: 1188–1190. - PubMed
-
- Miyata T, Takahama M, Yamamoto R, et al.. Sclerosing mediastinitis mimicking anterior mediastinal tumor. Ann Thorac Surg 2009; 88: 293–295. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
