

Biologic Therapy for Inflammatory Bowel Disease: Real-World Comparative Effectiveness and Impact of Drug Sequencing in 13 222 Patients within the UK IBD BioResource
- PMID: 38041850
- PMCID: PMC11147798
- DOI: 10.1093/ecco-jcc/jjad203
Biologic Therapy for Inflammatory Bowel Disease: Real-World Comparative Effectiveness and Impact of Drug Sequencing in 13 222 Patients within the UK IBD BioResource
Abstract
Background and aims: This study compares the effectiveness of different biologic therapies and sequences in patients with inflammatory bowel disease [IBD] using real-world data from a large cohort with long exposure.
Methods: Demographic, disease, treatment, and outcome data were retrieved for patients in the UK IBD BioResource. Effectiveness of treatment was based on persistence free of discontinuation or failure, analysed by Kaplan-Meier survival analysis with inverse probability of treatment weighting to adjust for differences between groups.
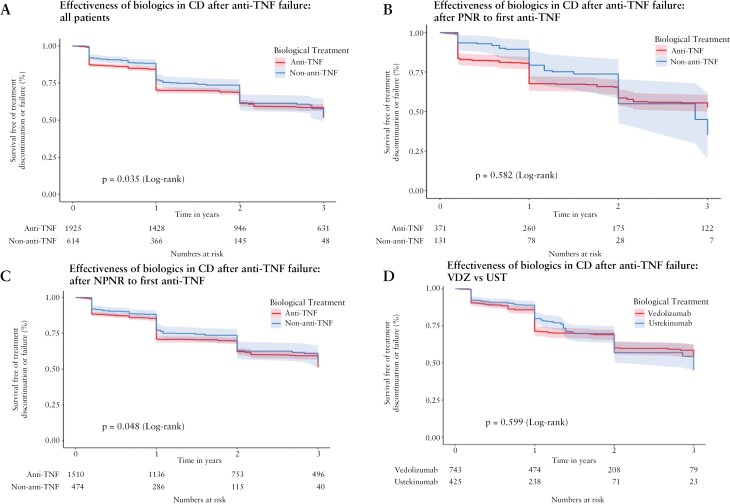
Results: In total, 13 222 evaluable patients received at least one biologic. In ulcerative colitis [UC] first-line vedolizumab [VDZ] demonstrated superior effectiveness over 5 years compared to anti-tumour necrosis factor [anti-TNF] agents [p = 0.006]. VDZ was superior to both infliximab [IFX] and adalimumab [ADA] after ADA and IFX failure respectively [p < 0.001 and p < 0.001]. Anti-TNF therapy showed similar effectiveness when used as first-line treatment, or after failure of VDZ. In Crohn's disease [CD] we found significant differences between first-line treatments over 10 years [p = 0.045], with superior effectiveness of IFX compared to ADA in perianal CD. Non-anti-TNF biologics were superior to a second anti-TNF after first-line anti-TNF failure in CD [p = 0.035]. Patients with UC or CD experiencing TNF failure due to delayed loss of response or intolerance had superior outcomes when switching to a non-anti-TNF biologic, rather than a second anti-TNF.
Conclusions: We provide real-world evidence to guide biologic selection and sequencing in a range of common scenarios. Our findings challenge current guidelines regarding drug selection after loss of response to first anti-TNF treatment.
Keywords: Crohn’s disease; biologic therapy; real-world effectiveness; sequencing; ulcerative colitis.
© The Author(s) 2023. Published by Oxford University Press on behalf of European Crohn’s and Colitis Organisation.
Conflict of interest statement
GWM is a consultant with Alimentiv and has active research funding from AstraZeneca, Bristol Myers Squibb, Alimentiv, and Johnson & Johnson. GWM has active research collaborations with Motilent. CAL receives research support and/or has received fees for delivery of education from: Genentech, Janssen, Takeda, Abbvie, Dr Falk, AstraZeneca, Eli Lilly, Orion, Pfizer, Roche, Sanofi Aventis, Ferring, UCB, Nordic Pharma, and Biogen. JKL has received research support from Galapagos and Takeda and speaker and consultancy fees from Abbvie, Arena, Bristol Myers Squibb, Celltrion, Eli Lilly, Ferring, Galapagos, Janssen, MSD, Pfizer, and Takeda. MP receives research funding from Pfizer, Galapagos, and AstraZeneca. TR has received research/educational grants and/or speaker/consultation fees from Abbvie, Arena, Aslan, AstraZeneca, Boehringer-Ingelheim, BMS, Celgene, Eli Lilly, Ferring, Galapagos, Gilead, GSK, Heptares, LabGenius, Janssen, Mylan, MSD, Novartis, Pfizer, Roche, Sandoz, Takeda, UCB, and XAP therapeutics. PMI reports research grants from Celltrion, Pfizer, Takeda, and Galapagos; consulting fees from AbbVie, Arena, Boehringer-Ingelheim, BMS, Celltrion, Elasmogen, Gilead, Janssen, Lilly, Pfizer, Prometheus, and Sandoz; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from AbbVie, BMS, Celgene, Celltrion, Falk Pharma, Galapagos, Gilead, Janssen, Lilly, Pfizer, Takeda, and Tillotts; and support for attending meetings and/or travel from Abbvie and Tillotts Pharma. SS has received speaker fees from Abbvie, Dr Falk pharmaceuticals, Takeda, Janssen, Celltrion,and Bristol-Myers Squibb, received educational grants from Abbvie, Takeda, and Janssen, and is an advisory board member for Abbvie, Dr Falk pharmaceuticals, Vifor pharmaceuticals, Janssen, Takeda, and Celltrion. SS is an associate editor for AP&T. RD received research support from Pfizer. CK, DL, EAS, KB, HP, LP, JR, JB, and JRN declare no conflict of interest.
Figures





Comment in
-
Real-world Positioning and Effectiveness of First- and Second-Line Biological Therapy in Inflammatory Bowel Diseases.J Crohns Colitis. 2024 Jun 3;18(6):787-789. doi: 10.1093/ecco-jcc/jjae001. J Crohns Colitis. 2024. PMID: 38233095 No abstract available.
References
-
- Sands BE, Irving PM, Hoops T, et al.; SEAVUE Study Group. Ustekinumab versus adalimumab for induction and maintenance therapy in biologic-naive patients with moderately to severely active Crohn’s disease: a multicentre, randomised, double-blind, parallel-group, phase 3b trial. Lancet 2022;399:2200–11. doi:10.1016/S0140-6736(22)00688-2 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
