

Influenza Vaccine Effectiveness Against Influenza A-Associated Emergency Department, Urgent Care, and Hospitalization Encounters Among US Adults, 2022-2023
- PMID: 39052725
- PMCID: PMC11306194
- DOI: 10.1093/infdis/jiad542
Influenza Vaccine Effectiveness Against Influenza A-Associated Emergency Department, Urgent Care, and Hospitalization Encounters Among US Adults, 2022-2023
Abstract
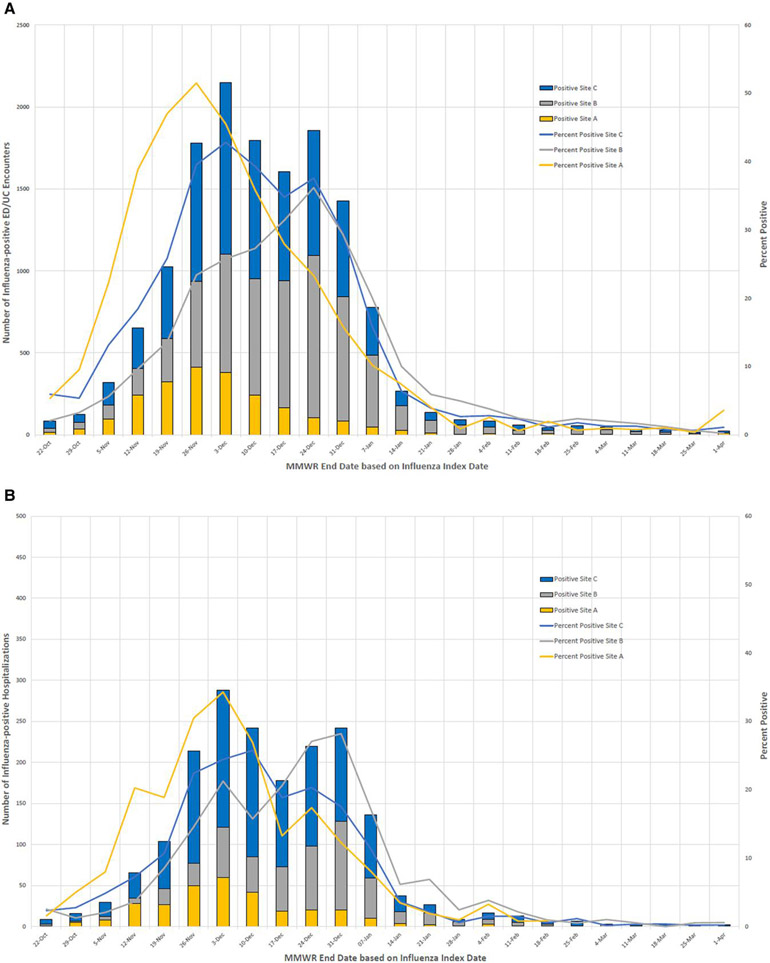
Background: The 2022-2023 United States influenza season had unusually early influenza activity with high hospitalization rates. Vaccine-matched A(H3N2) viruses predominated, with lower levels of A(H1N1)pdm09 activity also observed.
Methods: Using the test-negative design, we evaluated influenza vaccine effectiveness (VE) during the 2022-2023 season against influenza A-associated emergency department/urgent care (ED/UC) visits and hospitalizations from October 2022 to March 2023 among adults (aged ≥18 years) with acute respiratory illness (ARI). VE was estimated by comparing odds of seasonal influenza vaccination among case-patients (influenza A test positive by molecular assay) and controls (influenza test negative), applying inverse-propensity-to-be-vaccinated weights.
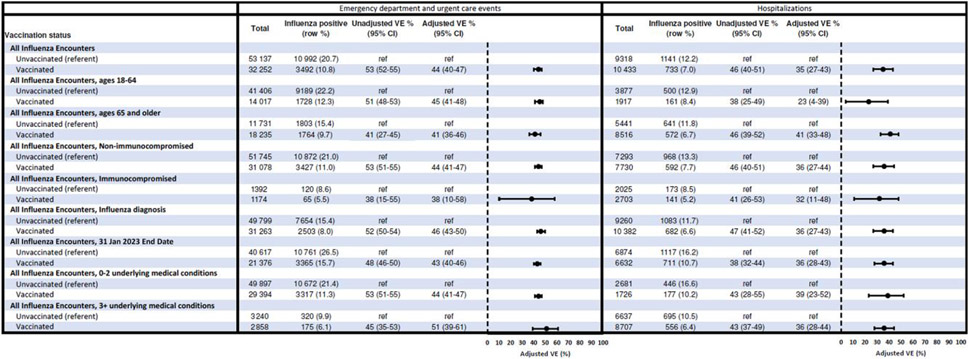
Results: The analysis included 85 389 ED/UC ARI encounters (17.0% influenza A positive; 37.8% vaccinated overall) and 19 751 hospitalizations (9.5% influenza A positive; 52.8% vaccinated overall). VE against influenza A-associated ED/UC encounters was 44% (95% confidence interval [CI], 40%-47%) overall and 45% and 41% among adults aged 18-64 and ≥65 years, respectively. VE against influenza A-associated hospitalizations was 35% (95% CI, 27%-43%) overall and 23% and 41% among adults aged 18-64 and ≥65 years, respectively.
Conclusions: VE was moderate during the 2022-2023 influenza season, a season characterized with increased burden of influenza and co-circulation with other respiratory viruses. Vaccination is likely to substantially reduce morbidity, mortality, and strain on healthcare resources.
Keywords: H3N2; clinical outcomes; influenza; test-negative design; vaccine effectiveness.
Published by Oxford University Press on behalf of Infectious Diseases Society of America 2023.
Conflict of interest statement
Potential conflicts of interest. During the conduct of the study, all Westat- and Kaiser Permanente Northern California Division of Research–affiliated authors reported receiving contractual support from the CDC via payments made to their respective institutions. Additionally, all authors affiliated with Baylor Scott & White Health, Children's Minnesota, Columbia University Irving Medical Center, HealthPartners Institute, Intermountain Healthcare, Kaiser Permanente Center for Health Research, Regenstrief Institute, University of Colorado Anschutz Medical Campus, and Vanderbilt University Medical Center reported receiving contractual support from the CDC during the conduct of the study, via subcontracts from Westat, Inc, with payments made to their respective institutions. Unrelated to the submitted work, the following disclosures were reported from the past 36 months: A. L. N. received grants from Pfizer and Vir Biotechnology; M. N. received grants directly from CDC and from CDC via subcontracts from Abt Associates and Vanderbilt University Medical Center to her institution; C. E. M. received grants AstraZeneca; S. R. received grants from GSK; and N. P. K. received research support from Pfizer, Merck, GlaxoSmithKline, Sanofi Pasteur, and Seqirus. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Centers for Disease Control and Prevention. Health Alert Network (HAN). Increased respiratory virus activity, especially among children, early in the 2022–2023 fall and winter. 2022. https://emergency.cdc.gov/han/2022/han00479.asp. Accessed 8 November 2022.
-
- Centers for Disease Control and Prevention. Influenza activity in the United States during the 2022–23 season and composition of the 2023–24 influenza vaccine. 2023. https://www.cdc.gov/flu/spotlights/2023-2024/22-23-summary-technical-rep.... Accessed 30 October 2023.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
