

CNS Efficacy of Osimertinib With or Without Chemotherapy in Epidermal Growth Factor Receptor-Mutated Advanced Non-Small-Cell Lung Cancer
- PMID: 38042525
- PMCID: PMC10906563
- DOI: 10.1200/JCO.23.02219
CNS Efficacy of Osimertinib With or Without Chemotherapy in Epidermal Growth Factor Receptor-Mutated Advanced Non-Small-Cell Lung Cancer
Abstract
Purpose: We report CNS efficacy of first-line osimertinib plus chemotherapy versus osimertinib monotherapy in patients with epidermal growth factor receptor (EGFR)-mutated advanced non-small-cell lung cancer (NSCLC) from the phase III FLAURA2 study according to baseline CNS metastasis status.
Methods: Patients were randomly assigned to osimertinib plus platinum-pemetrexed (combination) or osimertinib monotherapy until disease progression or discontinuation. Brain scans were performed in all patients at baseline and progression and at scheduled assessments until progression for patients with baseline CNS metastases; scans were assessed by neuroradiologist CNS blinded independent central review (BICR).
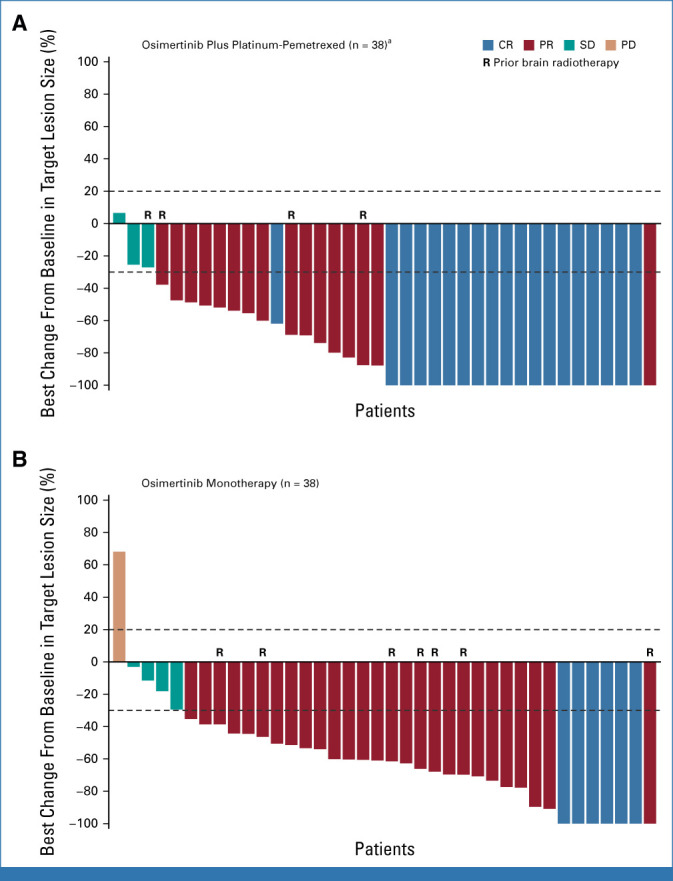
Results: On the basis of baseline CNS BICR, 118 of 279 (combination) and 104 of 278 (monotherapy) randomly assigned patients had ≥one measurable and/or nonmeasurable CNS lesion and were included in the CNS full analysis set (cFAS); 40 of 118 and 38 of 104 had ≥one measurable target CNS lesion and were included in the post hoc CNS evaluable-for-response set (cEFR). In the cFAS, the hazard ratio (HR) for CNS progression or death was 0.58 (95% CI, 0.33 to 1.01). In patients without baseline CNS metastases, the HR for CNS progression or death was 0.67 (95% CI, 0.43 to 1.04). In the cFAS, CNS objective response rates (ORRs; 95% CI) were 73% (combination; 64 to 81) versus 69% (monotherapy; 59 to 78); 59% versus 43% had CNS complete response (CR). In the cEFR, CNS ORRs (95% CI) were 88% (73 to 96) versus 87% (72 to 96); 48% versus 16% had CNS CR.
Conclusion: Osimertinib plus platinum-pemetrexed demonstrated improved CNS efficacy compared with osimertinib monotherapy, including delaying CNS progression, irrespective of baseline CNS metastasis status. These data support this combination as a new first-line treatment for patients with EGFR-mutated advanced NSCLC, including those with CNS metastases.
Trial registration: ClinicalTrials.gov NCT04035486.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
Figures






Comment in
-
Osimertinib-chemotherapy synergy in EGFR-mutant NSCLC: advancing central nervous system control amidst toxicity considerations.Transl Cancer Res. 2025 Apr 30;14(4):2188-2191. doi: 10.21037/tcr-2024-2207. Epub 2025 Apr 24. Transl Cancer Res. 2025. PMID: 40386260 Free PMC article. No abstract available.
-
FLAURA2: evidence for escalated first-line therapy in EGFR-mutated non-small cell lung cancer with central nervous system metastases.Transl Cancer Res. 2025 Jun 30;14(6):3295-3301. doi: 10.21037/tcr-2024-2589. Epub 2025 Jun 13. Transl Cancer Res. 2025. PMID: 40687261 Free PMC article. No abstract available.
References
-
- Peters S, Bexelius C, Munk V, et al. : The impact of brain metastasis on quality of life, resource utilization and survival in patients with non-small-cell lung cancer. Cancer Treat Rev 45:139-162, 2016 - PubMed
-
- Popat S, Ahn MJ, Ekman S, et al. : Osimertinib for EGFR-mutant non-small-cell lung cancer central nervous system metastases: Current evidence and future perspectives on therapeutic strategies. Target Oncol 18:9-24, 2023 - PubMed
-
- Cho BC, Han JY, Kim SW, et al. : A phase 1/2 study of lazertinib 240 mg in patients with advanced EGFR T790M-positive NSCLC after previous EGFR tyrosine kinase inhibitors. J Thorac Oncol 17:558-567, 2022 - PubMed
-
- Saito R, Sugawara S, Ko R, et al. : Phase 2 study of osimertinib in combination with platinum and pemetrexed in patients with previously untreated EGFR-mutated advanced non-squamous non-small cell lung cancer: The OPAL study. Eur J Cancer 185:83-93, 2023 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
