

Relationship between disproportionately enlarged subarachnoid-space hydrocephalus and white matter tract integrity in normal pressure hydrocephalus
- PMID: 38044360
- PMCID: PMC10694135
- DOI: 10.1038/s41598-023-48940-6
Relationship between disproportionately enlarged subarachnoid-space hydrocephalus and white matter tract integrity in normal pressure hydrocephalus
Abstract
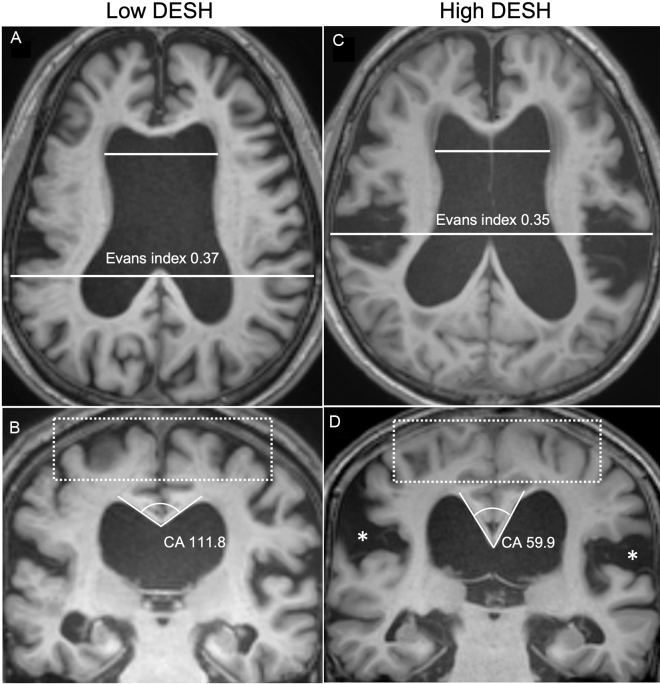
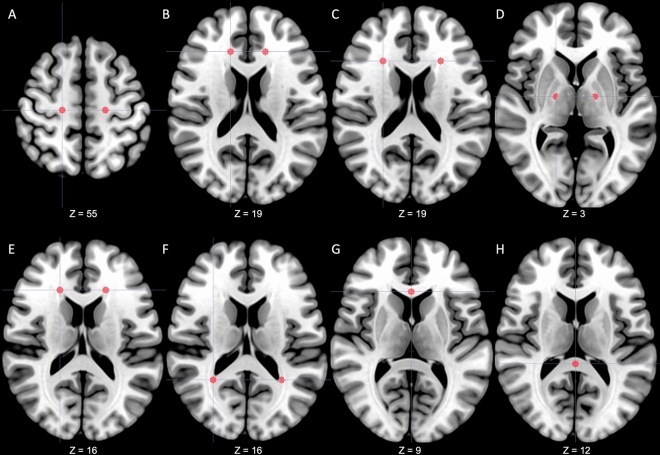
Normal pressure hydrocephalus (NPH) patients had altered white matter tract integrities on diffusion tensor imaging (DTI). Previous studies suggested disproportionately enlarged subarachnoid space hydrocephalus (DESH) as a prognostic sign of NPH. We examined DTI indices in NPH subgroups by DESH severity and clinical symptoms. This retrospective case-control study included 33 NPH patients and 33 age-, sex-, and education-matched controls. The NPH grading scales (0-12) were used to rate neurological symptoms. Patients with NPH were categorized into two subgroups, high-DESH and low-DESH groups, by the average value of the DESH scale. DTI indices, including fractional anisotropy, were compared across 14 regions of interest (ROIs). The high-DESH group had increased axial diffusivity in the lateral side of corona radiata (1.43 ± 0.25 vs. 1.72 ± 0.25, p = 0.04), and showed decreased fractional anisotropy and increased mean, and radial diffusivity in the anterior and lateral sides of corona radiata and the periventricular white matter surrounding the anterior horn of lateral ventricle. In patients with a high NPH grading scale, fractional anisotropy in the white matter surrounding the anterior horn of the lateral ventricle was significantly reduced (0.36 ± 0.08 vs. 0.26 ± 0.06, p = 0.03). These data show that DESH may be a biomarker for DTI-detected microstructural alterations and clinical symptom severity.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Garcia-Armengol R, et al. Comparison of elevated intracranial pressure pulse amplitude and disproportionately enlarged subarachnoid space (DESH) for prediction of surgical results in suspected idiopathic normal pressure hydrocephalus. Acta Neurochir. (Wien) 2016;158:2207–2213. doi: 10.1007/s00701-016-2858-5. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
