

Sellar Mass in 2 Patients With Acute-Onset Headache and Visual Symptoms: Not Your Usual Pituitary Adenoma
- PMID: 38045795
- PMCID: PMC10690422
- DOI: 10.1016/j.aace.2023.09.004
Sellar Mass in 2 Patients With Acute-Onset Headache and Visual Symptoms: Not Your Usual Pituitary Adenoma
Abstract
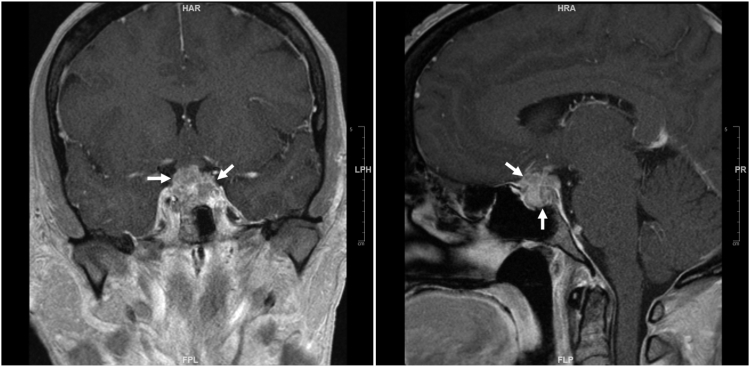
Background/objective: Clinical diagnosis of rare aggressive sellar malignancies requires a high index of suspicion. The objective was to report 2 patients with primary sellar atypical teratoid (AT)/rhabdoid tumor (RT) who presented with acute-onset headache and visual symptoms.
Case report: Patient 1 was a 45-year-old woman who presented with 3 weeks of headache and 1 week of eye pain and diplopia. Magnetic resonance imaging (MRI) identified a 2.2-cm sellar mass. Pituitary hormone testing showed elevated prolactin and suppressed luteinizing hormone, follicle-stimulating hormone, and estradiol levels. Patient 2 was a 32-year-old woman who presented with 1 month of headache and 1 week of diplopia. MRI showed a 2.1-cm sellar mass. Hormonal test results were reportedly unremarkable. Both patients did not have a significant medical history. They each underwent transsphenoidal resection. Surgical histology and molecular studies were consistent with primary sellar AT/RT. After surgery, patient 1 developed bilateral blindness and was lost to follow-up. Patient 2 developed hypopituitarism; her visual symptoms improved temporarily but recurred 2 weeks later. Pituitary MRI showed sellar recurrence. She underwent further debulking, but the tumor recurred promptly again. Despite radiation therapy, she died 4 months after the original presentation.
Discussion: AT/RT appears to be the most aggressive sellar malignancy.
Conclusion: Based on the 2 cases presented and the literature, I conclude that rapidly progressive headache with subsequent visual impairment in women with large sellar masses is almost pathognomonic of sellar AT/RT.
Keywords: acute-onset headache and visual symptoms; atypical teratoid/rhabdoid tumor; sellar compression symptoms; sellar mass.
© 2023 AACE. Published by Elsevier Inc.
Conflict of interest statement
The author has no multiplicity of interest to disclose.
Figures

References
-
- Schwetye K.E., Dahiya S.M. Sellar tumors. Surg Pathol Clin. 2020;13(2):305–329. - PubMed
-
- Jipa A., Jain V. Imaging of the sellar and parasellar regions. Clin Imaging. 2021;77:254–275. - PubMed
-
- Lev I., Fan X., Yu R. Sellar atypical teratoid/rhabdoid tumor: any preoperative diagnostic clues? AACE Clin Case Rep. 2015;1(1):e2–e7.