

Pathophysiology and surgical decision-making in central cord syndrome and degenerative cervical myelopathy: correcting the somatotopic fallacy
- PMID: 38046579
- PMCID: PMC10690824
- DOI: 10.3389/fneur.2023.1276399
Pathophysiology and surgical decision-making in central cord syndrome and degenerative cervical myelopathy: correcting the somatotopic fallacy
Abstract
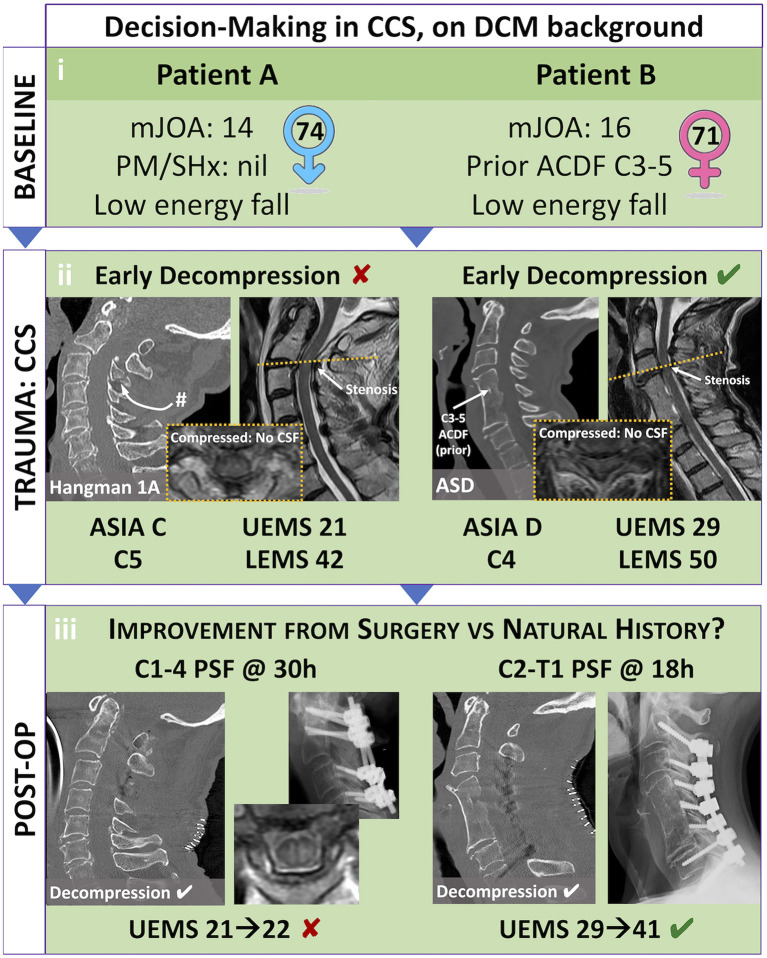
Our understanding of Central Cord Syndrome (CCS), a form of incomplete spinal cord injury characterized by disproportionate upper extremity weakness, is evolving. Recent advances challenge the traditional somatotopic model of corticospinal tract organization within the spinal cord, suggesting that CCS is likely a diffuse injury rather than focal lesion. Diagnostic criteria for CCS lack consensus, and varied definitions impact patient identification and treatment. Evidence has mounted for early surgery for CCS, although significant variability persists in surgical timing preferences among practitioners. A demographic shift toward an aging population has increased the overlap between CCS and Degenerative Cervical Myelopathy (DCM). Understanding this intersection is crucial for comprehensive patient care. Assessment tools, including quantitative measures and objective evaluations, aid in distinguishing CCS from DCM. The treatment landscape for CCS in the context of pre-existing DCM is complex, requiring careful consideration of pre-existing neurologic injury, patient factors, and injury factors. This review synthesizes emerging evidence, outlines current guidelines in diagnosis and management, and emphasizes the need for ongoing research to refine our understanding and treatment strategies for this evolving patient population.
Keywords: central cord syndrome; cervical spine; clinical outcome; myelopathy; neurosurgery; operative management; spinal cord injury; surgical intervention.
Copyright © 2023 Shakil, Santaguida, Wilson, Farhadi, Levi and Wilcox.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Fehlings MG, Wilson JR, Kopjar B, Yoon ST, Arnold PM, Massicotte EM, et al. . Efficacy and safety of surgical decompression in patients with cervical spondylotic myelopathy: results of the aospine North America prospective multi-center study. J Bone Joint Surg Am. (2013) 95:1651–8. 10.2106/JBJS.L.00589 - DOI - PubMed
-
- GBD 2016 Traumatic Brain Injury and Spinal Cord Injury Collaborators . Global, regional, and national burden of traumatic brain injury and spinal cord injury, 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. (2019) 18(1):56-87. 10.1016/S1474-4422(18)30415-0 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources