

Role of Polyunsaturated Fat in Modifying Cardiovascular Risk Associated With Family History of Cardiovascular Disease: Pooled De Novo Results From 15 Observational Studies
- PMID: 38047387
- PMCID: PMC10798593
- DOI: 10.1161/CIRCULATIONAHA.123.065530
Role of Polyunsaturated Fat in Modifying Cardiovascular Risk Associated With Family History of Cardiovascular Disease: Pooled De Novo Results From 15 Observational Studies
Abstract
Background: It is unknown whether dietary intake of polyunsaturated fatty acids (PUFA) modifies the cardiovascular disease (CVD) risk associated with a family history of CVD. We assessed interactions between biomarkers of low PUFA intake and a family history in relation to long-term CVD risk in a large consortium.
Methods: Blood and tissue PUFA data from 40 885 CVD-free adults were assessed. PUFA levels ≤25th percentile were considered to reflect low intake of linoleic, alpha-linolenic, and eicosapentaenoic/docosahexaenoic acids (EPA/DHA). Family history was defined as having ≥1 first-degree relative who experienced a CVD event. Relative risks with 95% CI of CVD were estimated using Cox regression and meta-analyzed. Interactions were assessed by analyzing product terms and calculating relative excess risk due to interaction.
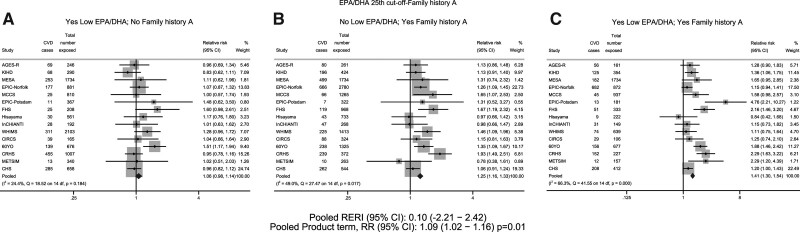
Results: After multivariable adjustments, a significant interaction between low EPA/DHA and family history was observed (product term pooled RR, 1.09 [95% CI, 1.02-1.16]; P=0.01). The pooled relative risk of CVD associated with the combined exposure to low EPA/DHA, and family history was 1.41 (95% CI, 1.30-1.54), whereas it was 1.25 (95% CI, 1.16-1.33) for family history alone and 1.06 (95% CI, 0.98-1.14) for EPA/DHA alone, compared with those with neither exposure. The relative excess risk due to interaction results indicated no interactions.
Conclusions: A significant interaction between biomarkers of low EPA/DHA intake, but not the other PUFA, and a family history was observed. This novel finding might suggest a need to emphasize the benefit of consuming oily fish for individuals with a family history of CVD.
Keywords: biomarkers; cardiovascular diseases; family medical history; polyunsaturated fatty acids; precision medicine.
Conflict of interest statement
Figures


References
-
- Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, Barengo NC, Beaton AZ, Benjamin EJ, Benziger CP, et al. ; GBD-NHLBI-JACC Global Burden of Cardiovascular Diseases Writing Group. Global burden of cardiovascular diseases and risk factors, 1990-2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76:2982–3021. doi: 10.1016/j.jacc.2020.11.010 - PMC - PubMed
-
- McClellan M, Brown N, Califf RM, Warner JJ. Call to action: urgent challenges in cardiovascular disease: a presidential advisory from the American Heart Association. Circulation. 2019;139:e44–e54. doi: 10.1161/CIR.0000000000000652 - PubMed
-
- Visseren FLJ, Mach F, Smulders YM, Carballo D, Koskinas KC, Back M, Benetos A, Biffi A, Boavida J-M, Capodanno D, et al. ; ESC National Cardiac Societies. 2021 ESC guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2021;42:3227–3337. doi: 10.1093/eurheartj/ehab484 - PubMed
-
- Arnett DK, Blumenthal RS, Albert MA, Buroker AB, Goldberger ZD, Hahn EJ, Himmelfarb CD, Khera A, Lloyd-Jones D, McEvoy JW, et al. . 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;140:e563–e595. doi: 10.1161/CIR.0000000000000677 - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
