

Cytomegalovirus Infection Facilitates the Costimulation of CD57+CD28- CD8 T Cells in HIV Infection and Atherosclerosis via the CD2-LFA-3 Axis
- PMID: 38047900
- PMCID: PMC10843654
- DOI: 10.4049/jimmunol.2300267
Cytomegalovirus Infection Facilitates the Costimulation of CD57+CD28- CD8 T Cells in HIV Infection and Atherosclerosis via the CD2-LFA-3 Axis
Abstract
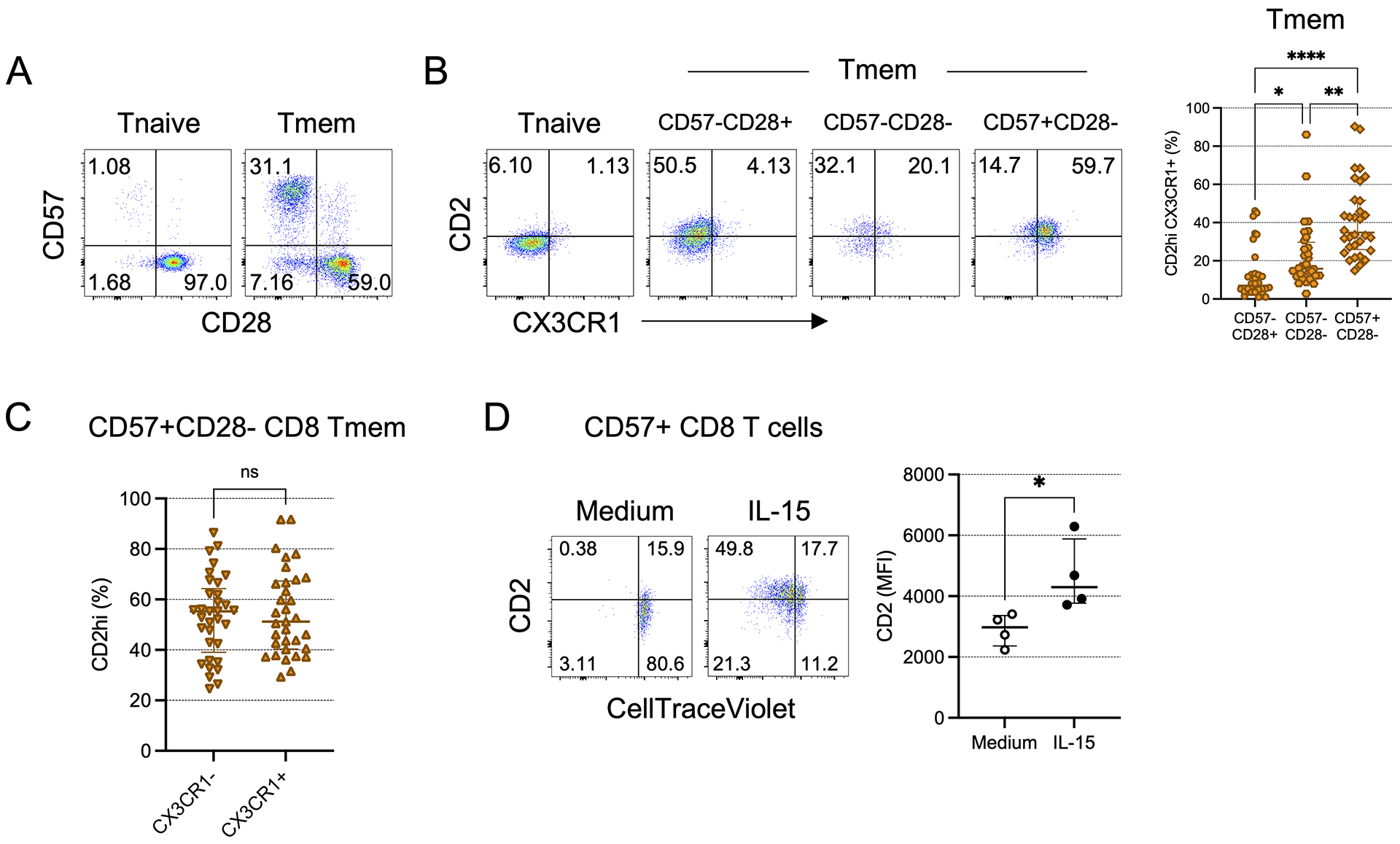
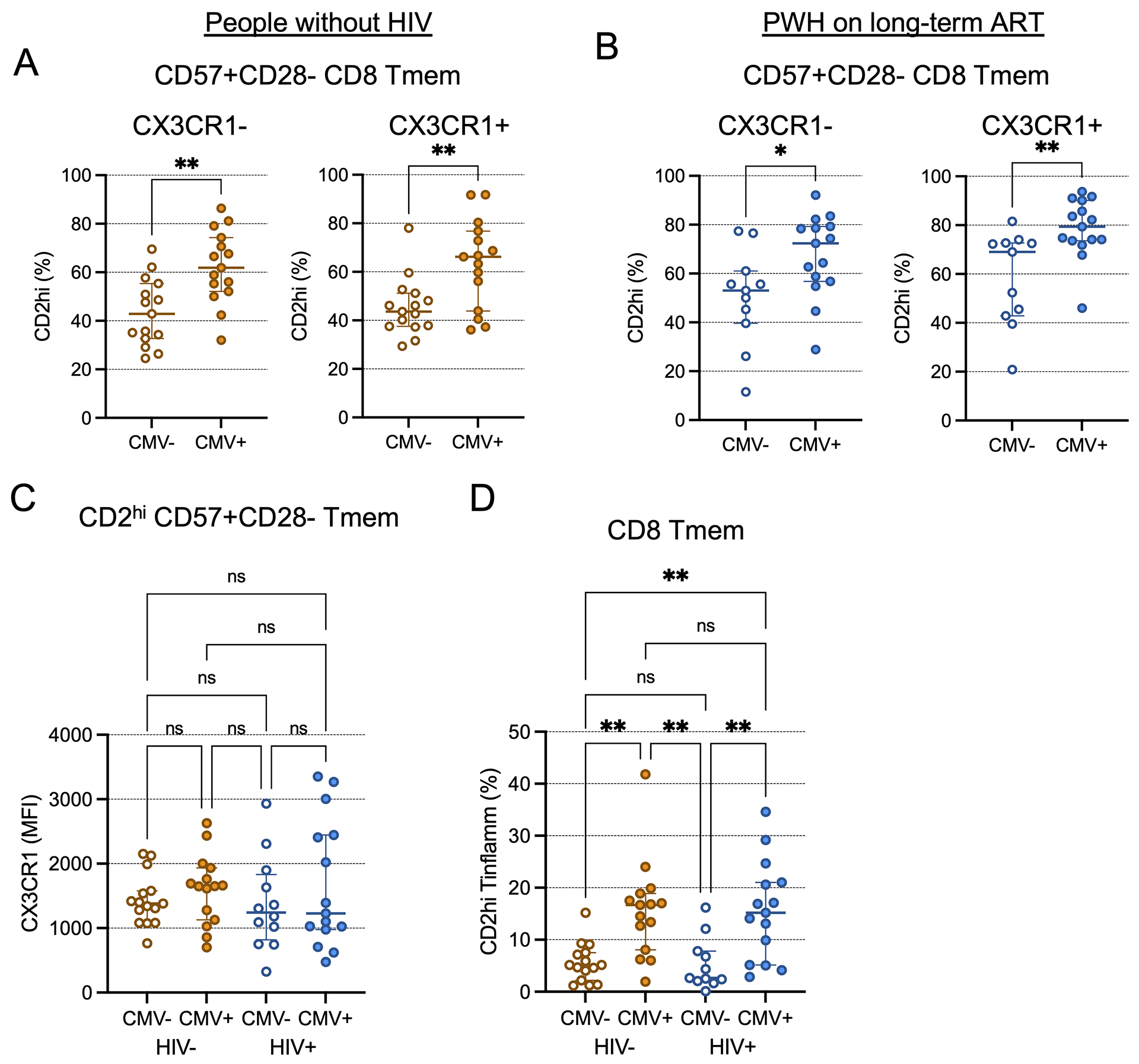
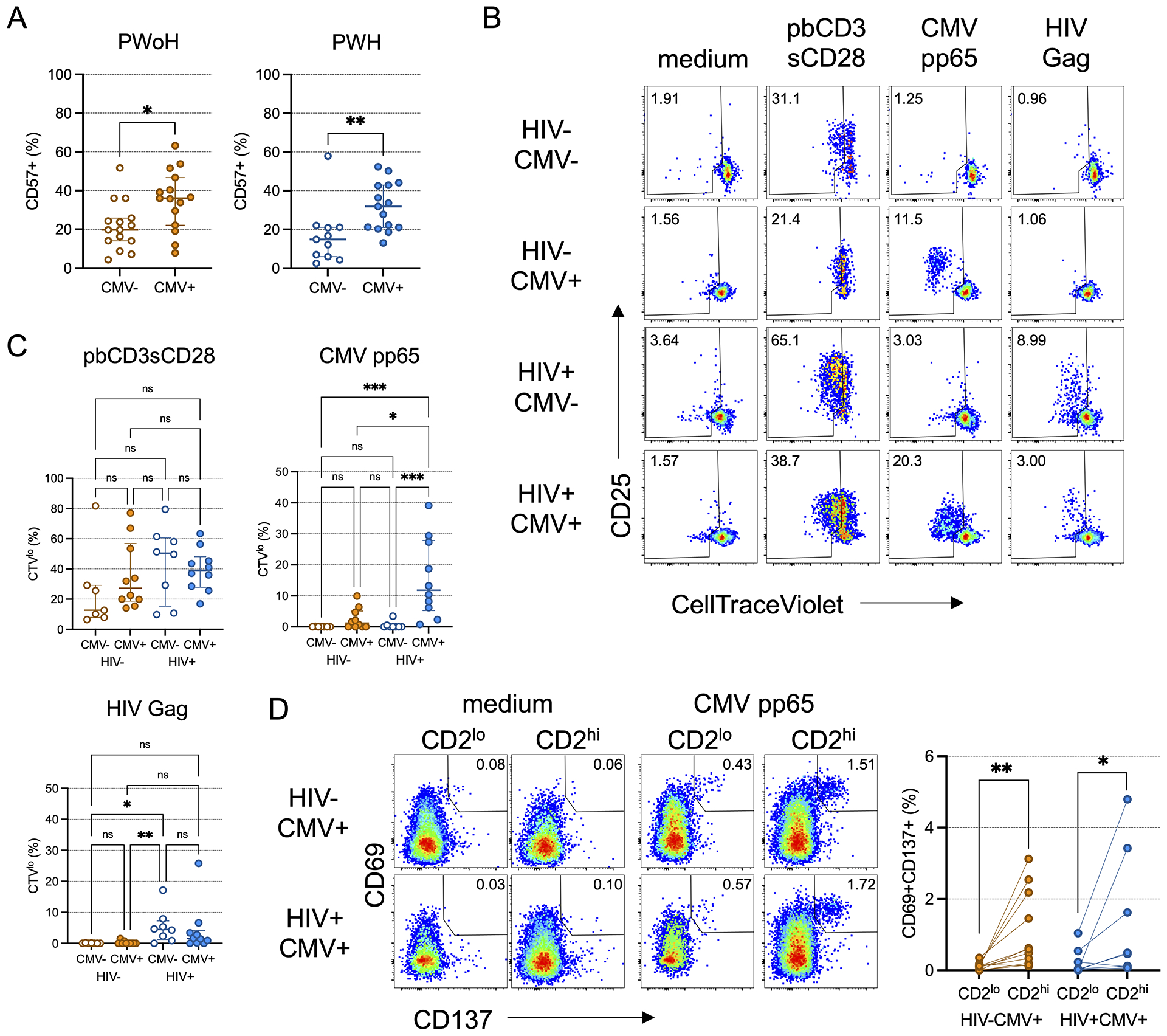
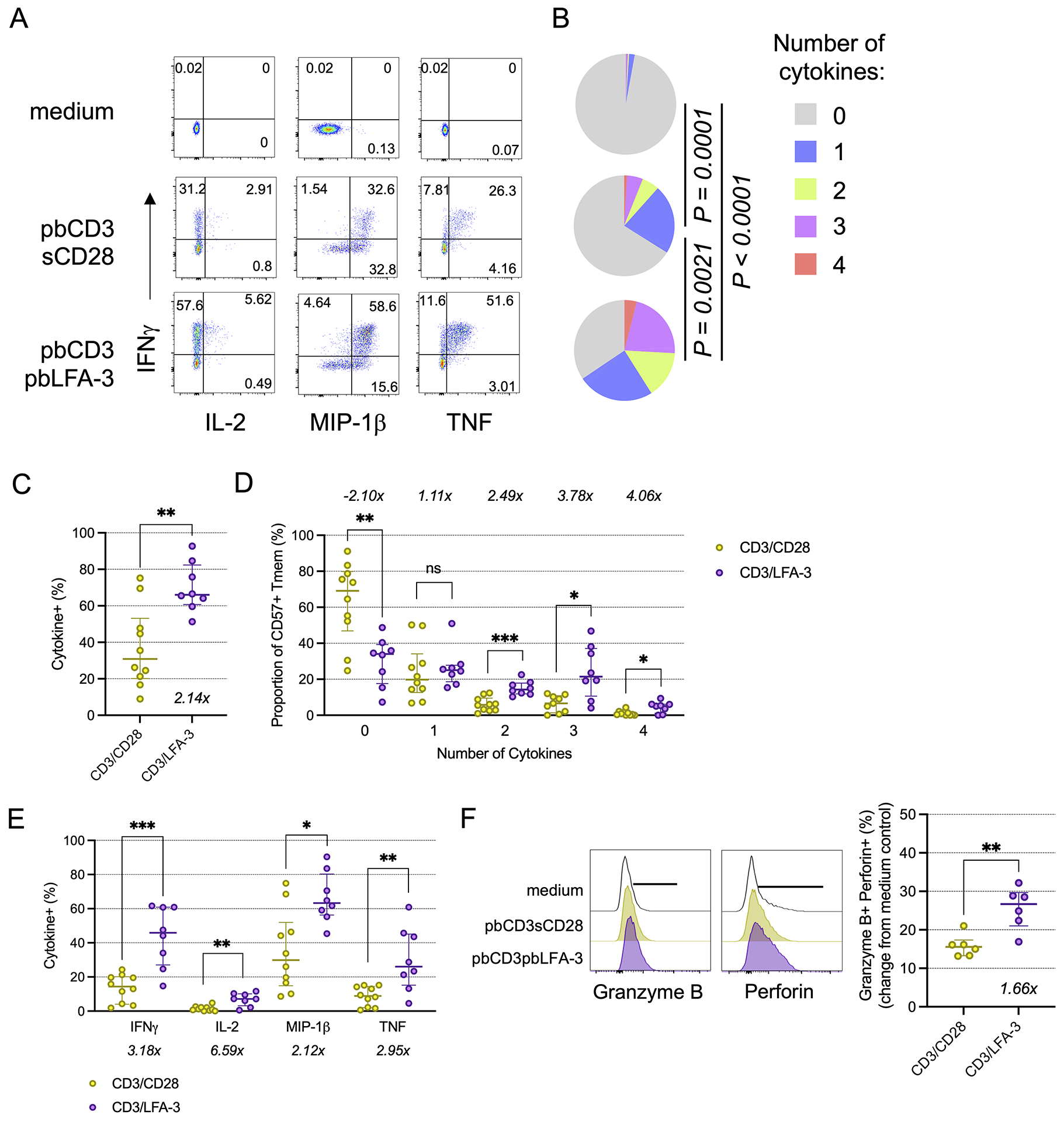
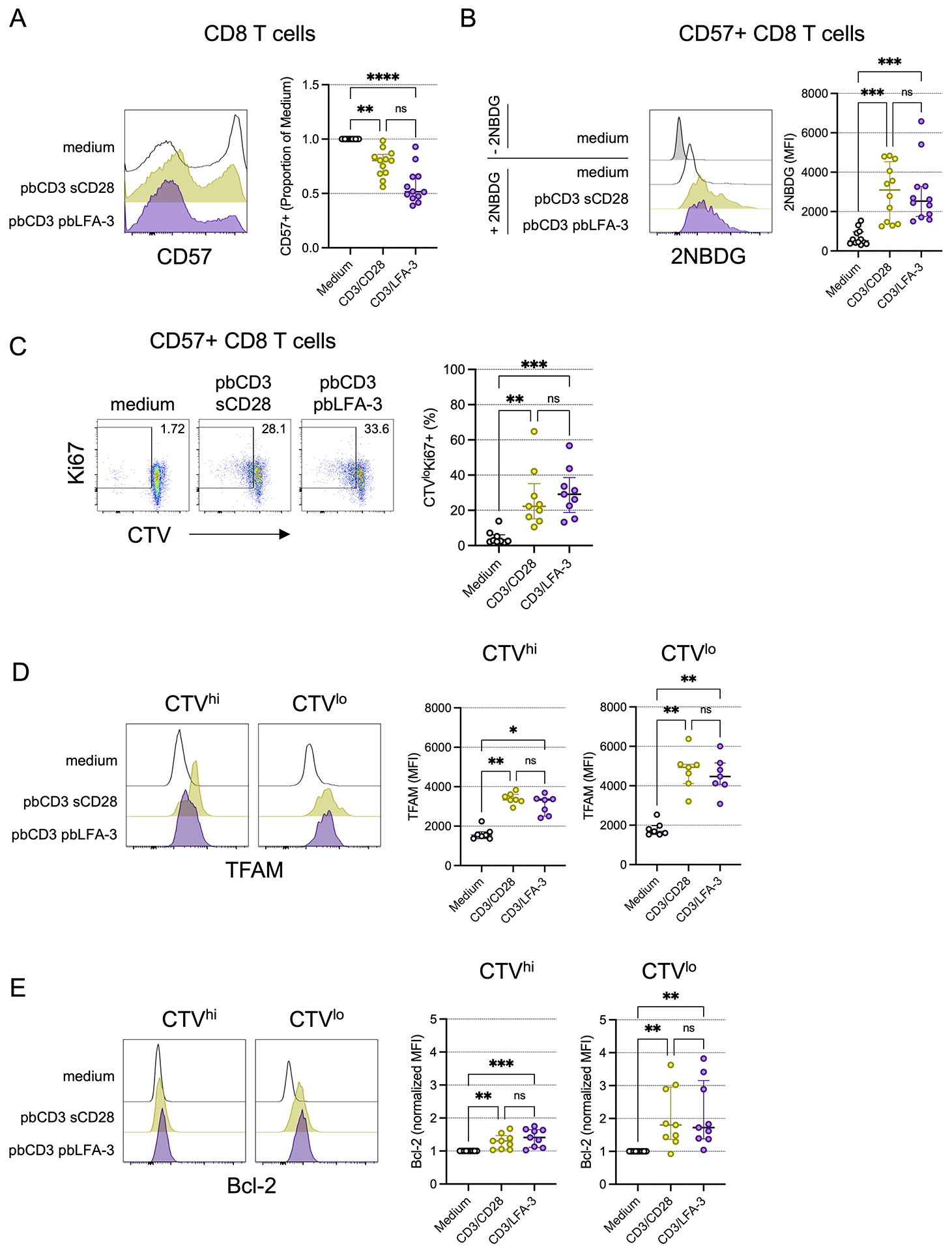
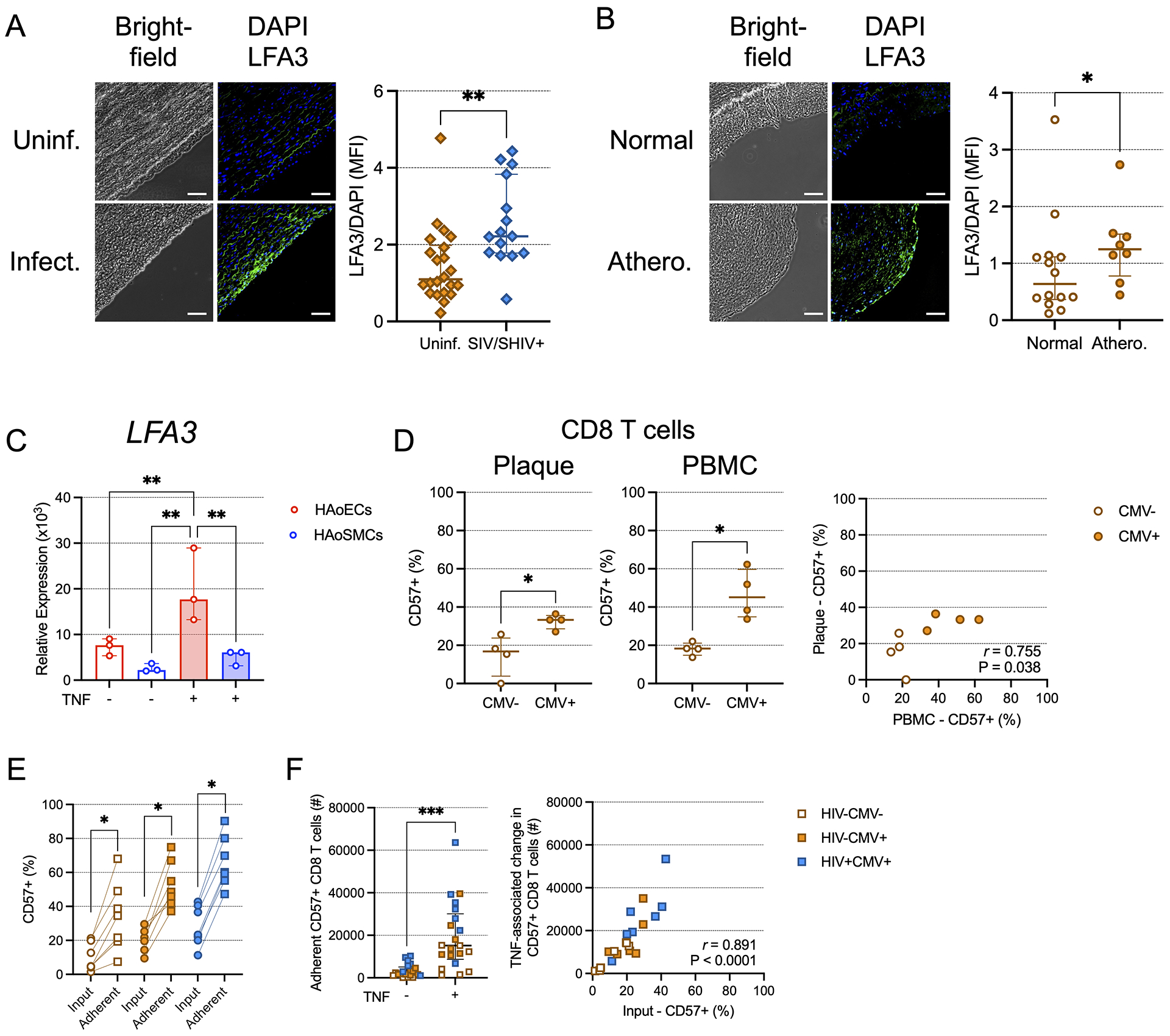
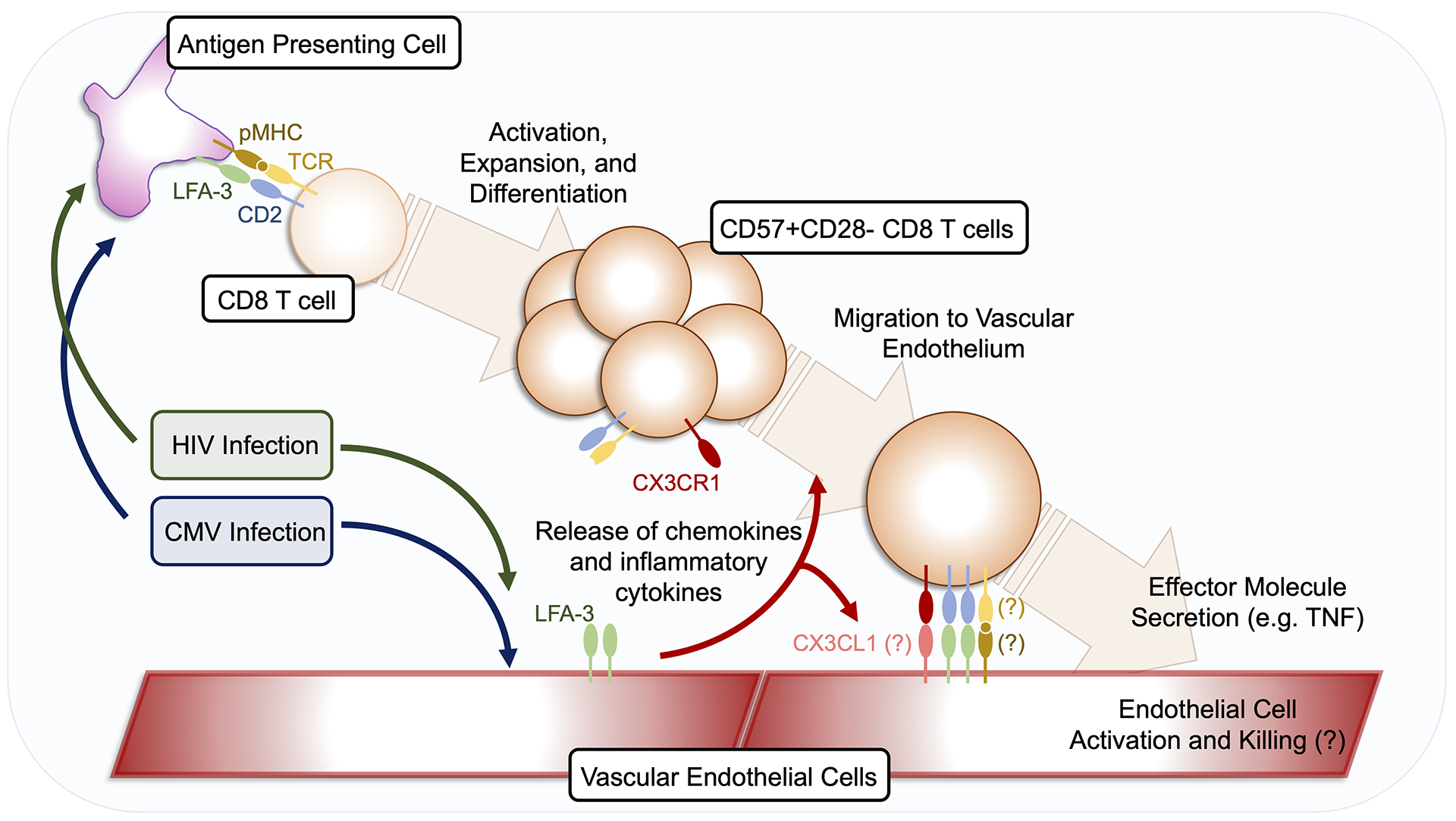
CD8 T cells are emerging as important mediators in atherosclerosis and cardiovascular disease (CVD). Immune activation may play a particular role in people with HIV (PWH) who are at an increased risk of CVD, even after controlling for known CVD risk factors. Latent CMV infection is associated with increased CVD risk for both PWH and people without HIV, and human CMV-specific CD4 and CD8 T cells are enriched for an immunosenescent phenotype. We previously showed that CMV coinfection in PWH promotes vascular homing and activation of inflammatory CD4 T cells through the CD2-LFA-3 axis. However, the role of CD2/LFA3 costimulation of CD8 T cells in PWH with CMV has yet to be described. In the present study, we demonstrate that CD2 expression on CX3CR1+CD57+CD28- inflammescent CD8 T cells is increased on cells from CMV-seropositive PWH. In vitro CD2/LFA-3 costimulation enhances TCR-mediated activation of these inflammatory CD8 memory T cells. Finally, we show that LFA-3 is highly expressed in aortas of SIV-infected rhesus macaques and in atherosclerotic plaques of people without HIV. Our findings are consistent with a model in which CMV infection enhances CD2 expression on highly proinflammatory CD8 T cells that can then be stimulated by LFA-3 expressed in the vasculature, even in the absence of CD28 costimulation. This model, in which CMV infection exacerbates toxic cytokine and granzyme production by CD8 T cells within the vasculature, highlights a potential therapeutic target in atherosclerosis development and progression, especially for PWH.
Copyright © 2024 by The American Association of Immunologists, Inc.
Conflict of interest statement
Dr. Lederman has received competitive funding from Gilead. The other authors have declared that no conflict of interest exists.
Figures
References
-
- Schouten J, Wit FW, Stolte IG, Kootstra NA, van der Valk M, Geerlings SE, Prins M, Reiss P, and Group AGCS. 2014. Cross-sectional comparison of the prevalence of age-associated comorbidities and their risk factors between HIV-infected and uninfected individuals: the AGEhIV cohort study. Clin Infect Dis 59: 1787–1797. - PubMed
-
- Shah ASV, Stelzle D, Lee KK, Beck EJ, Alam S, Clifford S, Longenecker CT, Strachan F, Bagchi S, Whiteley W, Rajagopalan S, Kottilil S, Nair H, Newby DE, McAllister DA, and Mills NL. 2018. Global Burden of Atherosclerotic Cardiovascular Disease in People Living With HIV: Systematic Review and Meta-Analysis. Circulation 138: 1100–1112. - PMC - PubMed
-
- Berry NJ, Burns DM, Wannamethee G, Grundy JE, Lui SF, Prentice HG, and Griffiths PD. 1988. Seroepidemiologic studies on the acquisition of antibodies to cytomegalovirus, herpes simplex virus, and human immunodeficiency virus among general hospital patients and those attending a clinic for sexually transmitted diseases. J Med Virol 24: 385–393. - PubMed
-
- Lang DJ, Kovacs AA, Zaia JA, Doelkin G, Niland JC, Aledort L, Azen SP, Fletcher MA, Gauderman J, Gjerset GJ, and et al. 1989. Seroepidemiologic studies of cytomegalovirus and Epstein-Barr virus infections in relation to human immunodeficiency virus type 1 infection in selected recipient populations. Transfusion Safety Study Group. J Acquir Immune Defic Syndr (1988) 2: 540–549. - PubMed
-
- Staras SA, Dollard SC, Radford KW, Flanders WD, Pass RF, and Cannon MJ. 2006. Seroprevalence of cytomegalovirus infection in the United States, 1988–1994. Clin Infect Dis 43: 1143–1151. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
