

Role of proton pump inhibitors dosage and duration in Helicobacter pylori eradication treatment: Results from the European Registry on H. pylori management
- PMID: 38050339
- PMCID: PMC10859719
- DOI: 10.1002/ueg2.12476
Role of proton pump inhibitors dosage and duration in Helicobacter pylori eradication treatment: Results from the European Registry on H. pylori management
Abstract
Background: Management of Helicobacter pylori (H. pylori) infection requires co-treatment with proton pump inhibitors (PPIs) and the use of antibiotics to achieve successful eradication.
Aim: To evaluate the role of dosage of PPIs and the duration of therapy in the effectiveness of H. pylori eradication treatments based on the 'European Registry on Helicobacter pylori management' (Hp-EuReg).
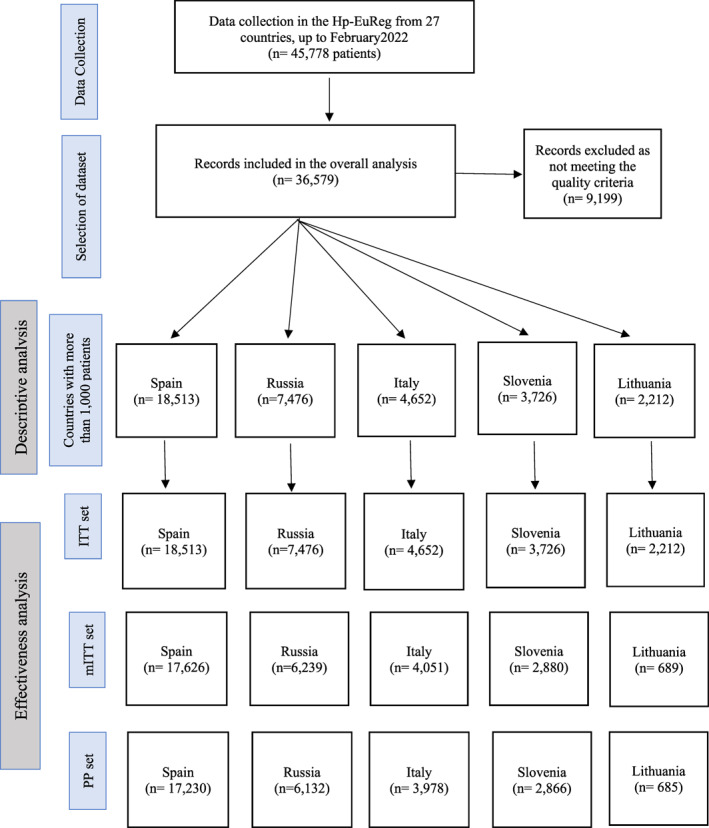
Methods: Hp-EuReg is a multicentre, prospective, non-interventionist, international registry on the routine clinical practice of H. pylori management by European gastroenterologists. All infected adult patients were systematically registered from 2013 to 2022.
Results: Overall, 36,579 patients from five countries with more than 1000 patients were analysed. Optimal (≥90%) first-line-modified intention-to-treat effectiveness was achieved with the following treatments: (1) 14-day therapies with clarithromycin-amoxicillin-bismuth and metronidazole-tetracycline-bismuth, both independently of the PPI dose prescribed; (2) All 10-day (except 10-day standard triple therapy) and 14-day therapies with high-dose PPIs; and (3) 10-day quadruple therapies with clarithromycin-amoxicillin-bismuth, metronidazole-tetracycline-bismuth, and clarithromycin-amoxicillin-metronidazole (sequential), all with standard-dose PPIs. In first-line treatment, optimal effectiveness was obtained with high-dose PPIs in all 14-day treatments, in 10- and 14-day bismuth quadruple therapies and in 10-day sequential with standard-dose PPIs. Optimal second-line effectiveness was achieved with (1) metronidazole-tetracycline-bismuth quadruple therapy for 14- and 10 days with standard and high-dose PPIs, respectively; and (2) levofloxacin-amoxicillin triple therapy for 14 days with high-dose PPIs. None of the 7-day therapies in both treatment lines achieved optimal effectiveness.
Conclusions: We recommend, in first-line treatment, the use of high-dose PPIs in 14-day triple therapy and in 10-or 14-day quadruple concomitant therapy in first-line treatment, while standard-dose PPIs would be sufficient in 10-day bismuth quadruple therapies. On the other hand, in second-line treatment, high-dose PPIs would be more beneficial in 14-day triple therapy with levofloxacin and amoxicillin or in 10-day bismuth quadruple therapy either as a three-in-one single capsule or in the traditional scheme.
Keywords: Helicobacter pylori; amoxicillin; bismuth; clarithromycin; levofloxacin; metronidazole; proton pump inhibitor; tetracycline; tinidazole; treatment.
© 2023 The Authors. United European Gastroenterology Journal published by Wiley Periodicals LLC. on behalf of United European Gastroenterology.
Conflict of interest statement
Dr. Javier P. Gisbert has served as a speaker, consultant, and advisory member for or has received research funding from Mayoly, Allergan, Diasorin, Gebro Pharma, and Richen. Dr. Olga P. Nyssen has received research funding from Mayoly and Allergan. The remaining authors declare no conflicts of interest.
Figures
References
-
- Malfertheiner P, Megraud F, Rokkas T, Gisbert JP, Liou JM, Schulz C, et al. Management of Helicobacter pylori infection‐the Maastricht VI/Florence Consensus Report. Gut. 2022;71(9):1724–1762. 10.1136/gutjnl-2022-327745 - DOI
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
