

Adenotonsillectomy for Snoring and Mild Sleep Apnea in Children: A Randomized Clinical Trial
- PMID: 38051326
- PMCID: PMC10698619
- DOI: 10.1001/jama.2023.22114
Adenotonsillectomy for Snoring and Mild Sleep Apnea in Children: A Randomized Clinical Trial
Abstract
Importance: The utility of adenotonsillectomy in children who have habitual snoring without frequent obstructive breathing events (mild sleep-disordered breathing [SDB]) is unknown.
Objectives: To evaluate early adenotonsillectomy compared with watchful waiting and supportive care (watchful waiting) on neurodevelopmental, behavioral, health, and polysomnographic outcomes in children with mild SDB.
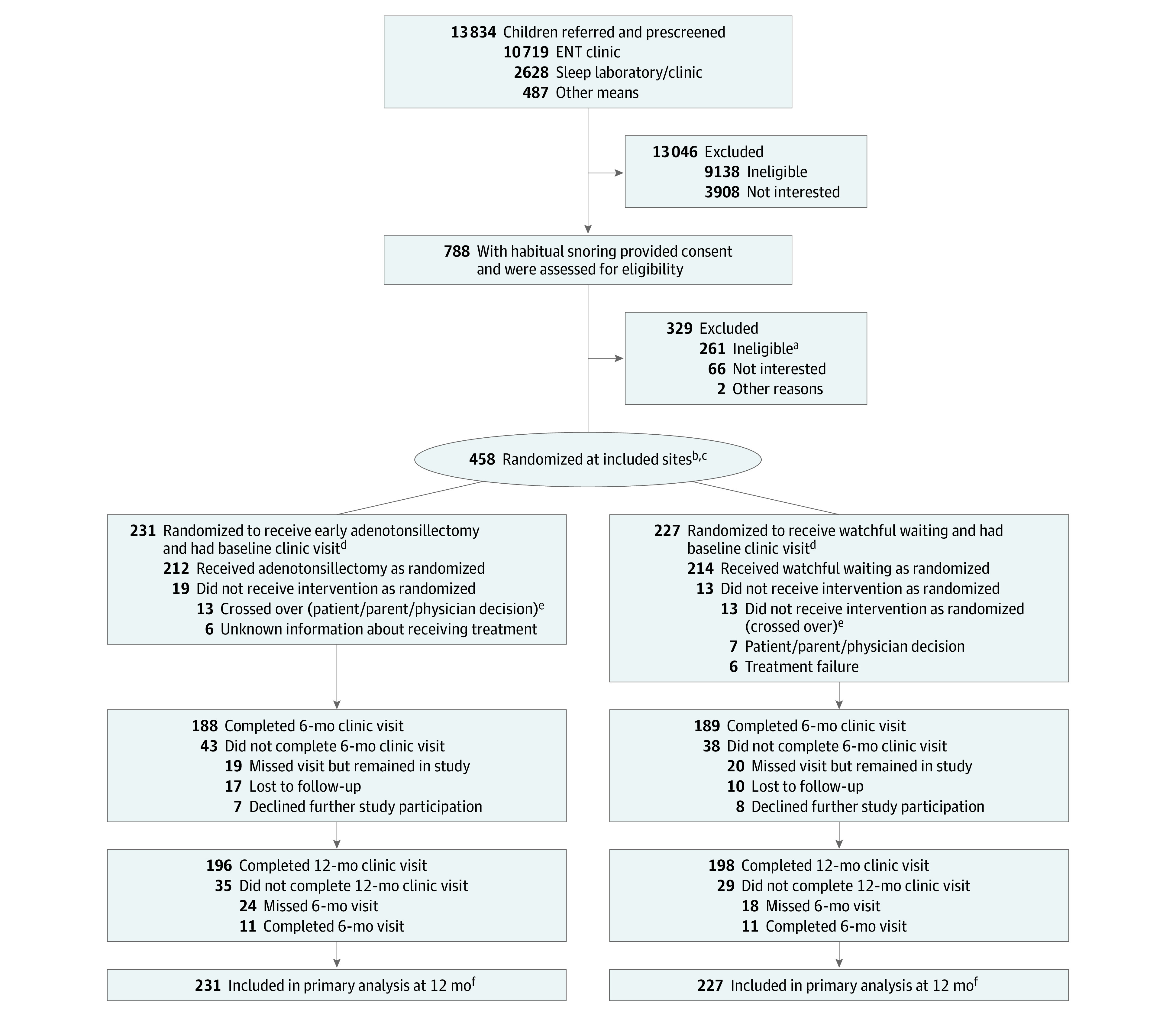
Design, setting, and participants: Randomized clinical trial enrolling 459 children aged 3 to 12.9 years with snoring and an obstructive apnea-hypopnea index (AHI) less than 3 enrolled at 7 US academic sleep centers from June 29, 2016, to February 1, 2021, and followed up for 12 months.
Intervention: Participants were randomized 1:1 to either early adenotonsillectomy (n = 231) or watchful waiting (n = 228).
Main outcomes and measures: The 2 primary outcomes were changes from baseline to 12 months for caregiver-reported Behavior Rating Inventory of Executive Function (BRIEF) Global Executive Composite (GEC) T score, a measure of executive function; and a computerized test of attention, the Go/No-go (GNG) test d-prime signal detection score, reflecting the probability of response to target vs nontarget stimuli. Twenty-two secondary outcomes included 12-month changes in neurodevelopmental, behavioral, quality of life, sleep, and health outcomes.
Results: Of the 458 participants in the analyzed sample (231 adenotonsillectomy and 237 watchful waiting; mean age, 6.1 years; 230 female [50%]; 123 Black/African American [26.9%]; 75 Hispanic [16.3%]; median AHI, 0.5 [IQR, 0.2-1.1]), 394 children (86%) completed 12-month follow-up visits. There were no statistically significant differences in change from baseline between the 2 groups in executive function (BRIEF GEC T-scores: -3.1 for adenotonsillectomy vs -1.9 for watchful waiting; difference, -0.96 [95% CI, -2.66 to 0.74]) or attention (GNG d-prime scores: 0.2 for adenotonsillectomy vs 0.1 for watchful waiting; difference, 0.05 [95% CI, -0.18 to 0.27]) at 12 months. Behavioral problems, sleepiness, symptoms, and quality of life each improved more with adenotonsillectomy than with watchful waiting. Adenotonsillectomy was associated with a greater 12-month decline in systolic and diastolic blood pressure percentile levels (difference in changes, -9.02 [97% CI, -15.49 to -2.54] and -6.52 [97% CI, -11.59 to -1.45], respectively) and less progression of the AHI to greater than 3 events/h (1.3% of children in the adenotonsillectomy group compared with 13.2% in the watchful waiting group; difference, -11.2% [97% CI, -17.5% to -4.9%]). Six children (2.7%) experienced a serious adverse event associated with adenotonsillectomy.
Conclusions: In children with mild SDB, adenotonsillectomy, compared with watchful waiting, did not significantly improve executive function or attention at 12 months. However, children with adenotonsillectomy had improved secondary outcomes, including behavior, symptoms, and quality of life and decreased blood pressure, at 12-month follow-up.
Trial registration: ClinicalTrials.gov Identifier: NCT02562040.
Conflict of interest statement
Figures
Comment in
-
Adenotonsillectomy or Watchful Waiting for Pediatric Sleep-Disordered Breathing.JAMA. 2023 Dec 5;330(21):2057-2058. doi: 10.1001/jama.2023.22373. JAMA. 2023. PMID: 38051336 No abstract available.
-
Skip Polysomnography Before Adenotonsillectomy for Snoring?JAMA Otolaryngol Head Neck Surg. 2024 Jun 1;150(6):528-529. doi: 10.1001/jamaoto.2024.0585. JAMA Otolaryngol Head Neck Surg. 2024. PMID: 38635260 No abstract available.
