

Senotherapeutic drug treatment ameliorates chemotherapy-induced cachexia
- PMID: 38051584
- PMCID: PMC10906225
- DOI: 10.1172/jci.insight.169512
Senotherapeutic drug treatment ameliorates chemotherapy-induced cachexia
Abstract
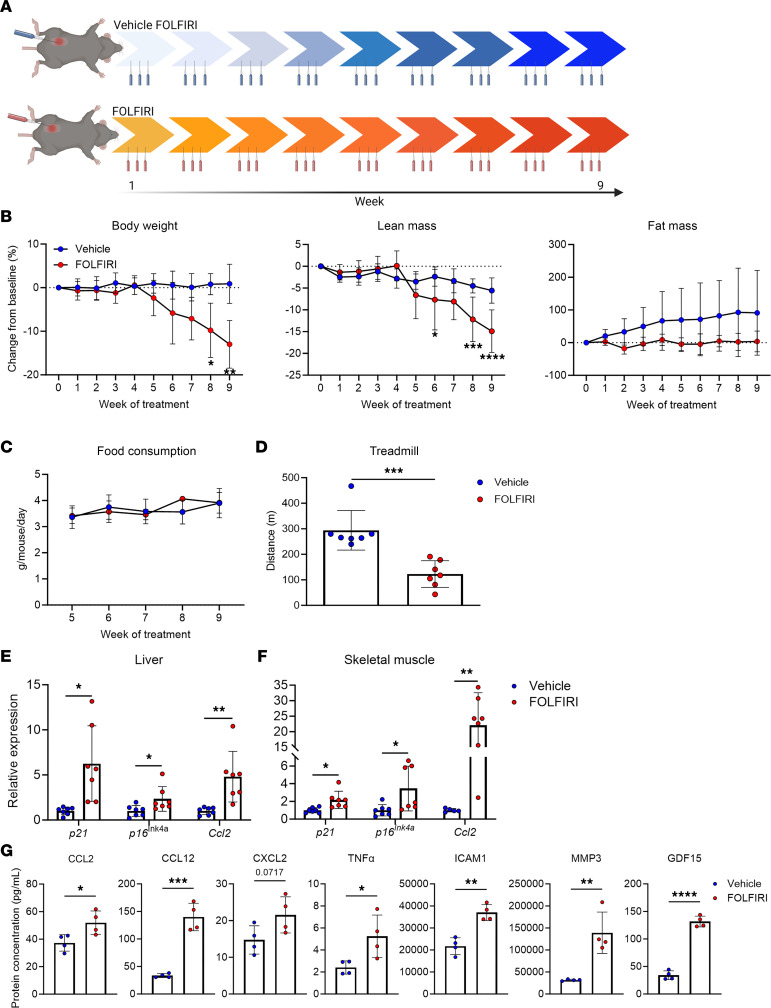
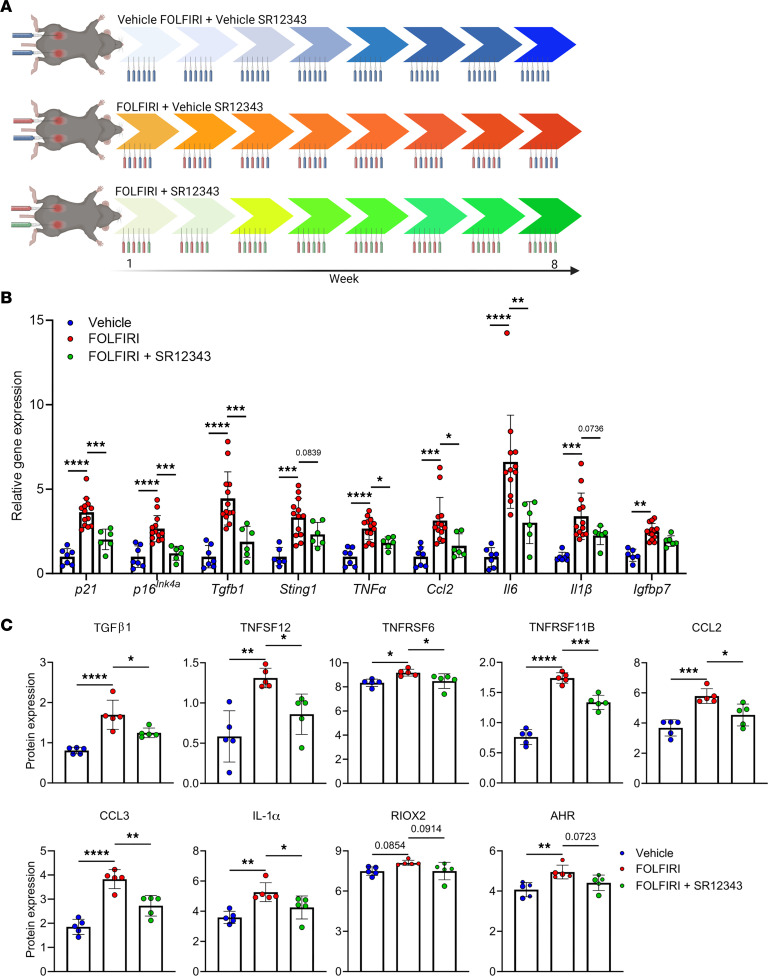
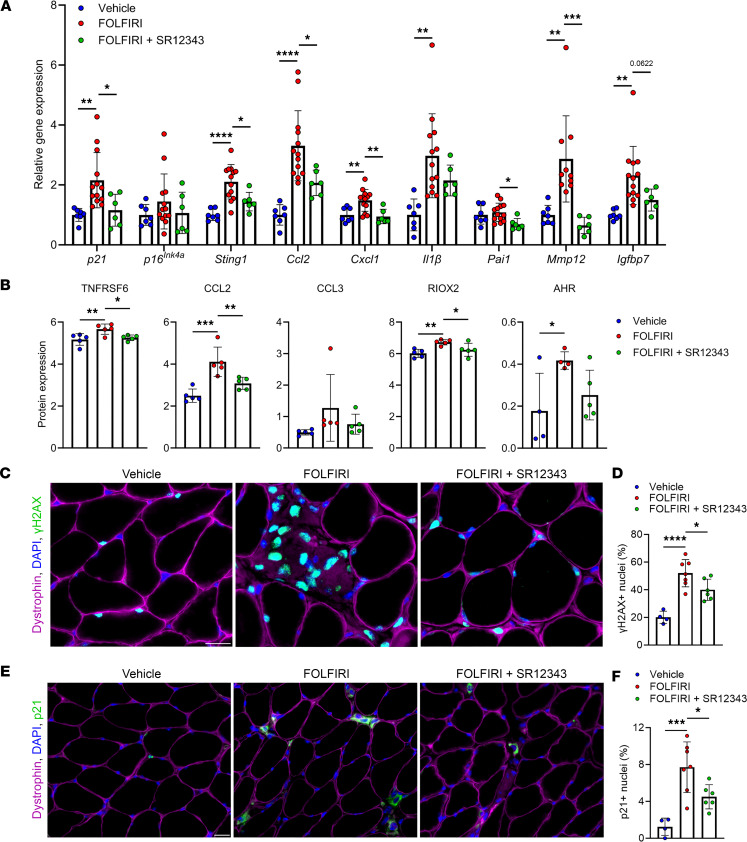
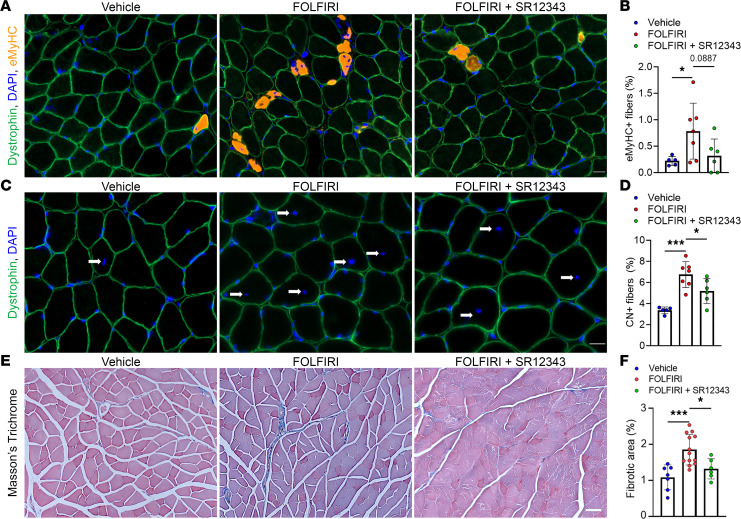
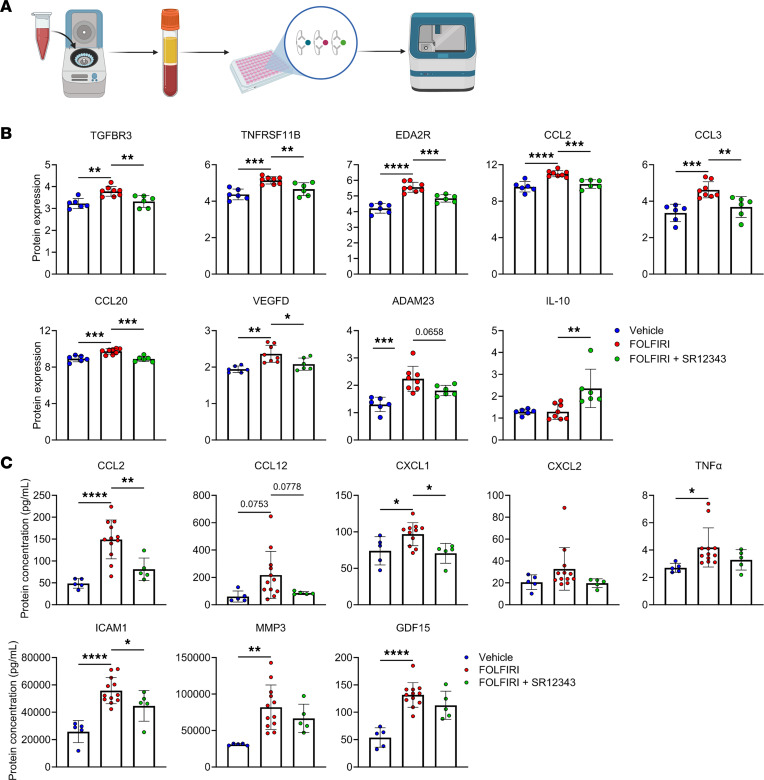
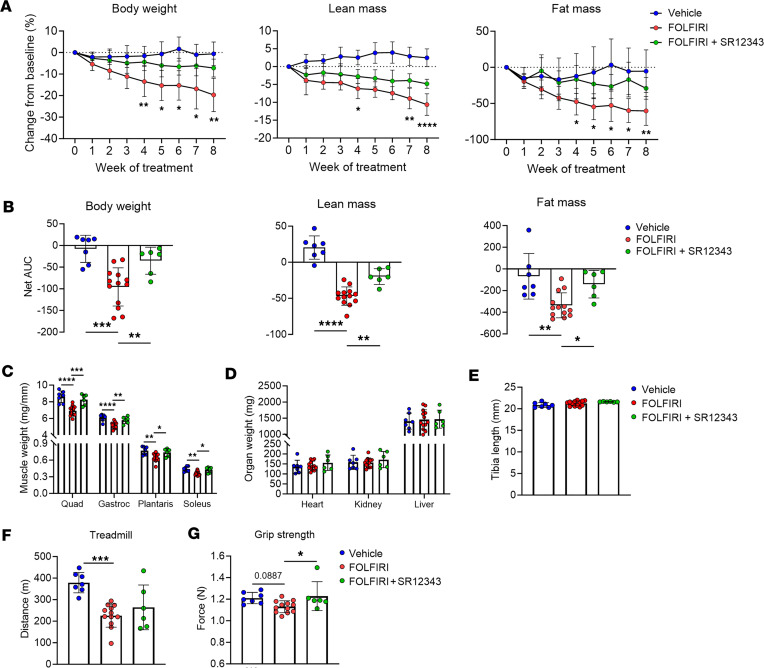
Cachexia is a debilitating skeletal muscle wasting condition for which we currently lack effective treatments. In the context of cancer, certain chemotherapeutics cause DNA damage and cellular senescence. Senescent cells exhibit chronic activation of the transcription factor NF-κB, a known mediator of the proinflammatory senescence-associated secretory phenotype (SASP) and skeletal muscle atrophy. Thus, targeting NF-κB represents a logical therapeutic strategy to alleviate unintended consequences of genotoxic drugs. Herein, we show that treatment with the IKK/NF-κB inhibitor SR12343 during a course of chemotherapy reduces markers of cellular senescence and the SASP in liver, skeletal muscle, and circulation and, correspondingly, attenuates features of skeletal muscle pathology. Lastly, we demonstrate that SR12343 mitigates chemotherapy-induced reductions in body weight, lean mass, fat mass, and muscle strength. These findings support senescent cells as a promising druggable target to counteract the SASP and skeletal muscle wasting in the context of chemotherapy.
Keywords: Cellular senescence; Inflammation; Muscle Biology; Skeletal muscle.
Conflict of interest statement
Figures
References
-
- Langstein HN, et al. The roles of gamma-interferon and tumor necrosis factor alpha in an experimental rat model of cancer cachexia. Cancer Res. 1991;51(9):2302–2306. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
