

Vaccine Effectiveness Against Influenza A-Associated Hospitalization, Organ Failure, and Death: United States, 2022-2023
- PMID: 38051664
- PMCID: PMC11487098
- DOI: 10.1093/cid/ciad677
Vaccine Effectiveness Against Influenza A-Associated Hospitalization, Organ Failure, and Death: United States, 2022-2023
Abstract
Background: Influenza circulation during the 2022-2023 season in the United States largely returned to pre-coronavirus disease 2019 (COVID-19)-pandemic patterns and levels. Influenza A(H3N2) viruses were detected most frequently this season, predominately clade 3C.2a1b.2a, a close antigenic match to the vaccine strain.
Methods: To understand effectiveness of the 2022-2023 influenza vaccine against influenza-associated hospitalization, organ failure, and death, a multicenter sentinel surveillance network in the United States prospectively enrolled adults hospitalized with acute respiratory illness between 1 October 2022, and 28 February 2023. Using the test-negative design, vaccine effectiveness (VE) estimates against influenza-associated hospitalization, organ failures, and death were measured by comparing the odds of current-season influenza vaccination in influenza-positive case-patients and influenza-negative, SARS-CoV-2-negative control-patients.
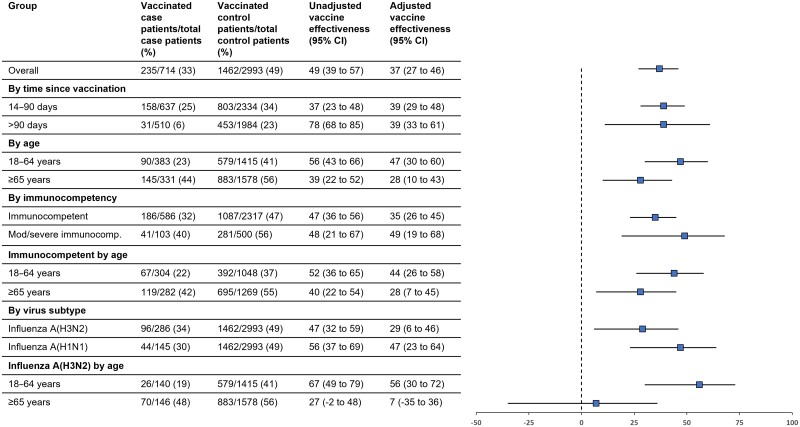
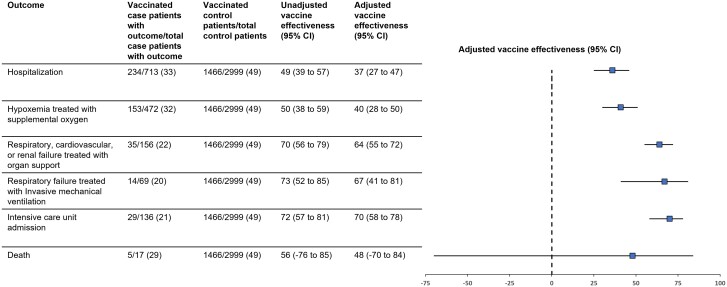
Results: A total of 3707 patients, including 714 influenza cases (33% vaccinated) and 2993 influenza- and severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)-negative controls (49% vaccinated) were analyzed. VE against influenza-associated hospitalization was 37% (95% confidence interval [CI]: 27%-46%) and varied by age (18-64 years: 47% [30%-60%]; ≥65 years: 28% [10%-43%]), and virus (A[H3N2]: 29% [6%-46%], A[H1N1]: 47% [23%-64%]). VE against more severe influenza-associated outcomes included: 41% (29%-50%) against influenza with hypoxemia treated with supplemental oxygen; 65% (56%-72%) against influenza with respiratory, cardiovascular, or renal failure treated with organ support; and 66% (40%-81%) against influenza with respiratory failure treated with invasive mechanical ventilation.
Conclusions: During an early 2022-2023 influenza season with a well-matched influenza vaccine, vaccination was associated with reduced risk of influenza-associated hospitalization and organ failure.
Keywords: acute respiratory illness; attenuation; influenza; organ failure; vaccine effectiveness.
Published by Oxford University Press on behalf of Infectious Diseases Society of America 2023.
Conflict of interest statement
Potential conflicts of interest. S. B. reports participating as the DSMB chair for Hamilton Ventilators, outside the submitted work. J. C. reports receiving funding from the National Institutes of Health (NIH) and Department of Defense (DoD), and a travel grant from Fisher-Paykel, outside the submitted work. S. C. reports consulting for PureTech Health in 2021–2022 and Kiniksa Pharmaceuticals in 2022, outside the submitted work. A. D. reports participating on an advisory board for ALung Technologies and being a principal investigator (PI) for the PETAL Network, outside the submitted work. C. G. G. reports consulting fees from Merck and received research support from Campbell Alliance/Syneos Health, NIH, CDC, Food and Drug Administration (FDA), and AHRQ, outside the submitted work. M. N. G. reports receiving grant funding from NIH and AHRQ for research, honorarium for giving Medicine grand rounds at Yale and Washington Healthcare, fees for DSMB for Palm trial and Regeneron trials on monoclonal antibodies, and fees for serving on scientific advisory board for Philips Healthcare on monitoring, outside the submitted work. R. G. reports consulting for Gilead Sciences, Eli Lily, GSK, Janssen, and AbbVie, being on an advisory board for Gilead Sciences, Eli Lily, GlaxoSmithKline (GSK), and AstraZeneca, speaker bureau for Pfizer and AbbVie, and gift-in-kind to institution from Gilead Sciences, outside the submitted work. N. H. reports prior grant support from Sanofi and Quidel, and current funding from Merck, outside the submitted work. A. L. reports being a consultant for Roche on a clinical trial of baloxavir, outside the submitted work. Christopher Mallow reports medical legal consulting, outside the submitted work. I. P. reports receiving grants from NHLBI, NIGMS, and Janssen Pharmaceuticals and institutional support from Regeneron, outside the submitted work. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- CDC . Fluview Past Weekly Surveillance Reports 2017–2023. Available at: https://www.cdc.gov/flu/weekly/pastreports.htm. Accessed 18 March 2023.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
