

The clinical utility of three frailty measures in identifying HIV-associated neurocognitive disorders
- PMID: 38051787
- PMCID: PMC10939888
- DOI: 10.1097/QAD.0000000000003805
The clinical utility of three frailty measures in identifying HIV-associated neurocognitive disorders
Abstract
Objective: Frailty measures vary widely and the optimal measure for predicting HIV-associated neurocognitive disorders (HAND) is unclear.
Design: A study was conducted to examine the clinical utility of three widely used frailty measures in identifying HIV-associated neurocognitive disorders.
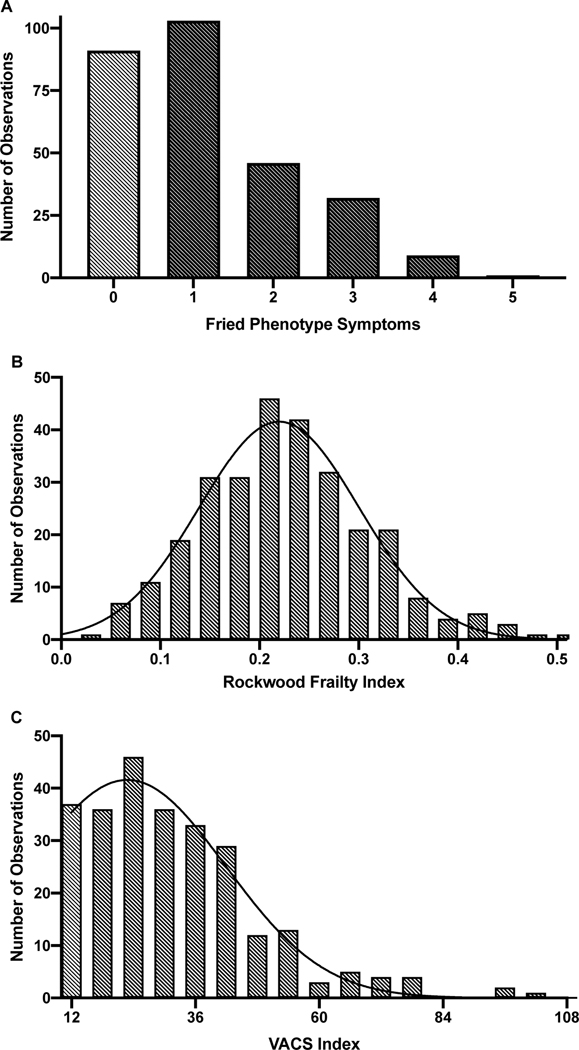
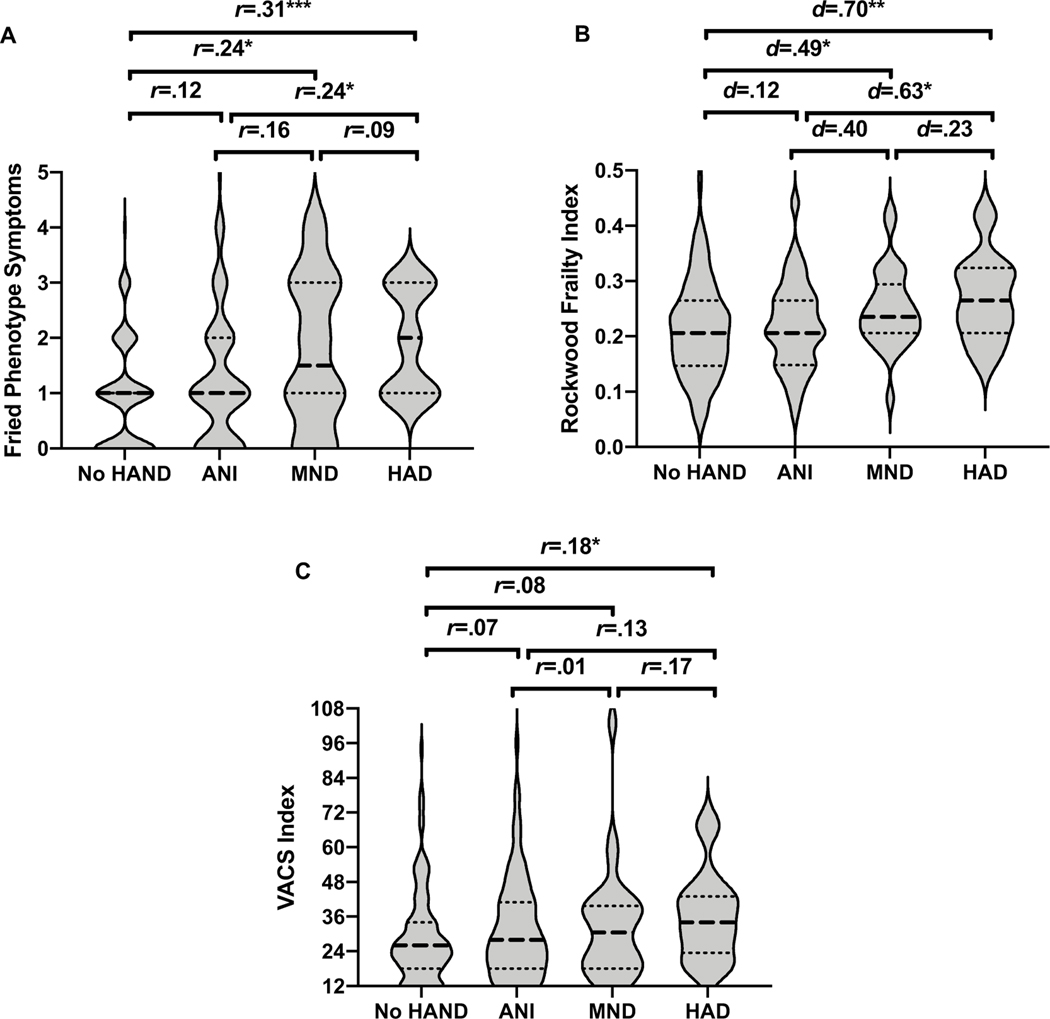
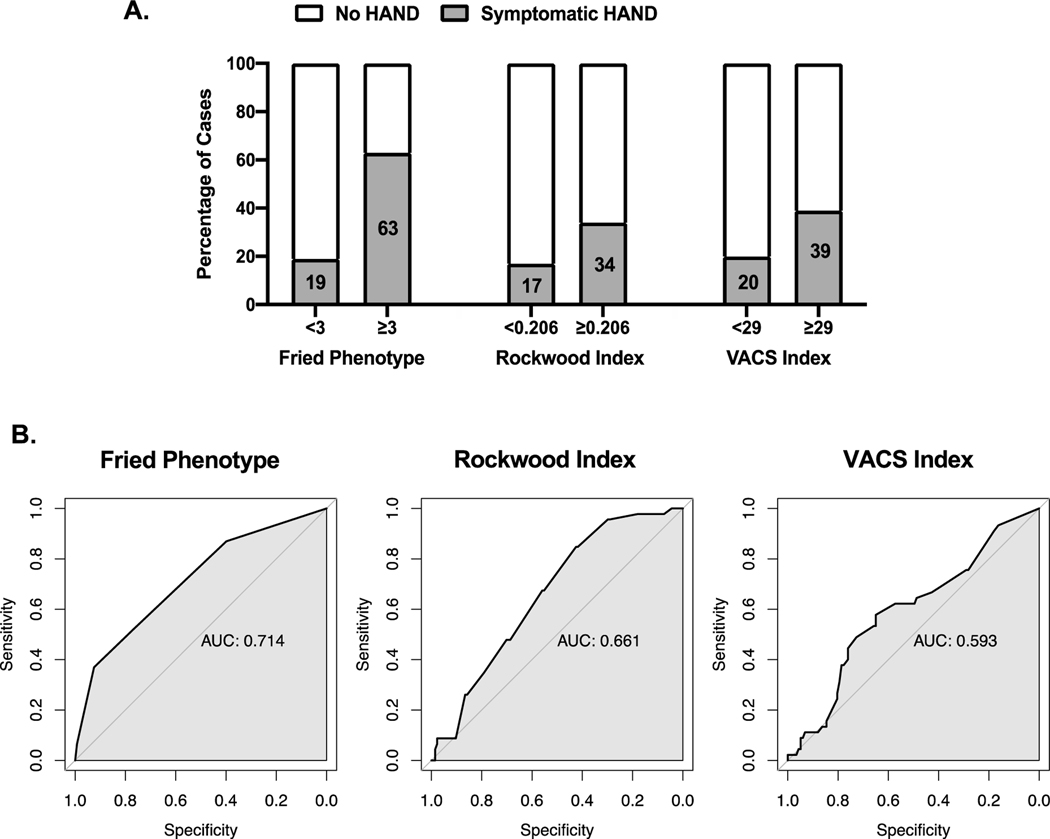
Methods: The study involved 284 people with HIV (PWH) at least 50 years enrolled at UC San Diego's HIV Neurobehavioral Research Program. Frailty measurements included the Fried Phenotype, the Rockwood Frailty Index, and the Veterans Aging Cohort Study (VACS) Index. HAND was diagnosed according to Frascati criteria. ANOVAs examined differences in frailty severity across HAND conditions. ROC analyses evaluated sensitivity and specificity of each measure to detect symptomatic HAND [mild neurocognitive disorder (MND) and HIV-associated dementia (HAD)] from no HAND.
Results: Across all frailty measures, frailty was found to be higher in HAD compared with no HAND. For Fried and Rockwood (not VACS), frailty was significantly more severe in MND vs. no HAND and in HAD vs. ANI (asymptomatic neurocognitive impairment). For discriminating symptomatic HAND from no HAND, Fried was 37% sensitive and 92% specific, Rockwood was 85% sensitive and 43% specific, and VACS was 58% sensitive and 65% specific.
Conclusion: These findings demonstrate that Fried and Rockwood outperform VACS in predicting HAND. However, ROC analyses suggest none of the indices had adequate predictive validity in detecting HAND. The results indicate that the combined use of the Rockwood and Fried indices may be an appropriate alternative.
Copyright © 2023 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Declaration of Interests
The authors do not have a commercial or other association that might pose a conflict of interest.
Figures
Comment in
-
Frailty and HIV-associated neurocognitive disorder are only modestly associated.AIDS. 2024 Apr 1;38(5):757-759. doi: 10.1097/QAD.0000000000003842. Epub 2024 Mar 14. AIDS. 2024. PMID: 38482907 Free PMC article. No abstract available.
Similar articles
-
Brief Report: Frailty and HIV Disease Severity Synergistically Increase Risk of HIV-Associated Neurocognitive Disorders.J Acquir Immune Defic Syndr. 2020 Aug 15;84(5):522-526. doi: 10.1097/QAI.0000000000002391. J Acquir Immune Defic Syndr. 2020. PMID: 32692111 Free PMC article.
-
Association Between Frailty and HIV-Associated Neurodegenerative Disorders Among Older Adults Living with HIV.AIDS Res Hum Retroviruses. 2018 May;34(5):449-455. doi: 10.1089/AID.2017.0100. Epub 2018 Mar 13. AIDS Res Hum Retroviruses. 2018. PMID: 29385834 Free PMC article.
-
The Veterans Aging Cohort Study Index is not associated with HIV-associated neurocognitive disorders in Uganda.J Neurovirol. 2020 Apr;26(2):252-256. doi: 10.1007/s13365-019-00806-2. Epub 2019 Nov 12. J Neurovirol. 2020. PMID: 31721082 Free PMC article.
-
Screening for HIV-Associated Neurocognitive Disorders: Sensitivity and Specificity.Curr Top Behav Neurosci. 2021;50:429-478. doi: 10.1007/7854_2019_117. Curr Top Behav Neurosci. 2021. PMID: 32677005 Review.
-
Considerations on nosology for HIV-associated neurocognitive disorders: it is time to update?Infection. 2020 Feb;48(1):37-42. doi: 10.1007/s15010-019-01373-8. Epub 2019 Nov 6. Infection. 2020. PMID: 31691905 Review.
Cited by
-
Frailty and HIV-associated neurocognitive disorder are only modestly associated.AIDS. 2024 Apr 1;38(5):757-759. doi: 10.1097/QAD.0000000000003842. Epub 2024 Mar 14. AIDS. 2024. PMID: 38482907 Free PMC article. No abstract available.
-
DNA methylation-based telomere length is associated with HIV infection, physical frailty, cancer, and all-cause mortality.Aging Cell. 2024 Jul;23(7):e14174. doi: 10.1111/acel.14174. Epub 2024 Apr 17. Aging Cell. 2024. PMID: 38629454 Free PMC article.
References
-
- de Vries NM, Staal JB, van Ravensberg CD, Hobbelen JSM, Olde Rikkert MGM, Nijhuis-van der Sanden MWG. Outcome instruments to measure frailty: A systematic review. Ageing Res Rev 2011; 10:104–114. - PubMed
-
- Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al. Frailty in Older Adults: Evidence for a Phenotype. Journals Gerontol Ser A Biol Sci Med Sci 2001; 56:M146–M157. - PubMed
-
- Rockwood K, Mitnitski A. Frailty in Relation to the Accumulation of Deficits. Journals Gerontol Ser A Biol Sci Med Sci 2007; 62:722–727. - PubMed
