

A comparative analysis of perioperative complications and biochemical recurrence between standard and extended pelvic lymph node dissection in prostate cancer patients undergoing radical prostatectomy: a systematic review and meta-analysis
- PMID: 38052016
- PMCID: PMC10942186
- DOI: 10.1097/JS9.0000000000000997
A comparative analysis of perioperative complications and biochemical recurrence between standard and extended pelvic lymph node dissection in prostate cancer patients undergoing radical prostatectomy: a systematic review and meta-analysis
Abstract
Introduction: Pelvic lymph node dissection (PLND) is commonly performed during radical prostatectomy (RP) for prostate cancer staging. This study aimed to comprehensively analyze existing evidence compare perioperative complications associated with standard (sPLND) versus extended PLND templates (ePLND) in RP patients.
Methods: A meta-analysis of prospective studies on PLND complications was conducted. Systematic searches were performed on Web of Science, Pubmed, Embase, and the Cochrane Library until May 2023. Risk ratios (RRs) were estimated using random-effects models in the meta-analysis. The statistical analysis of the data was carried out using Review Manager software.
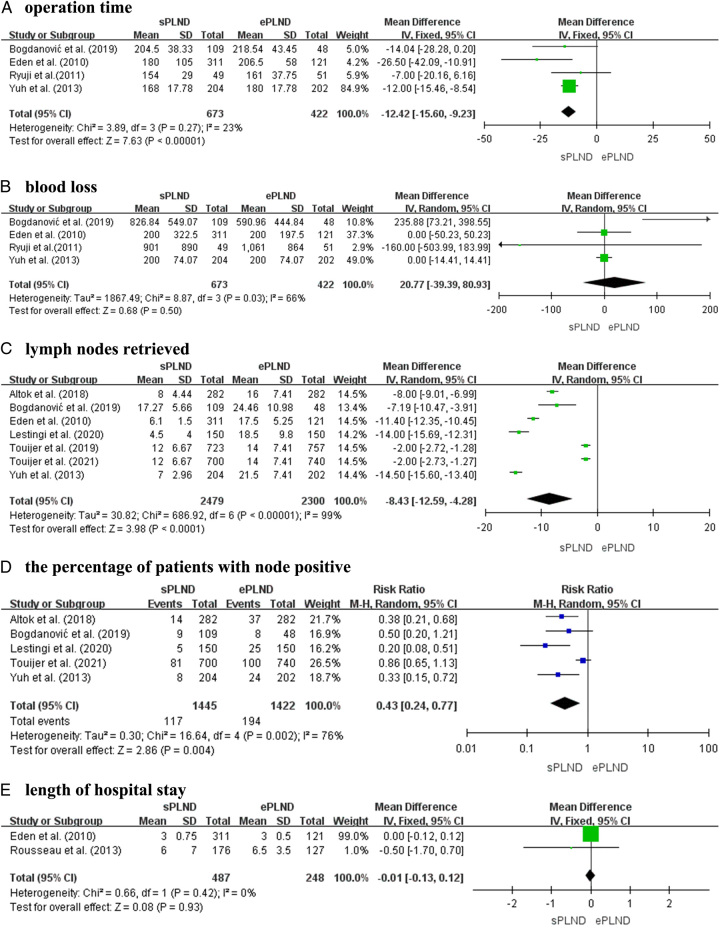
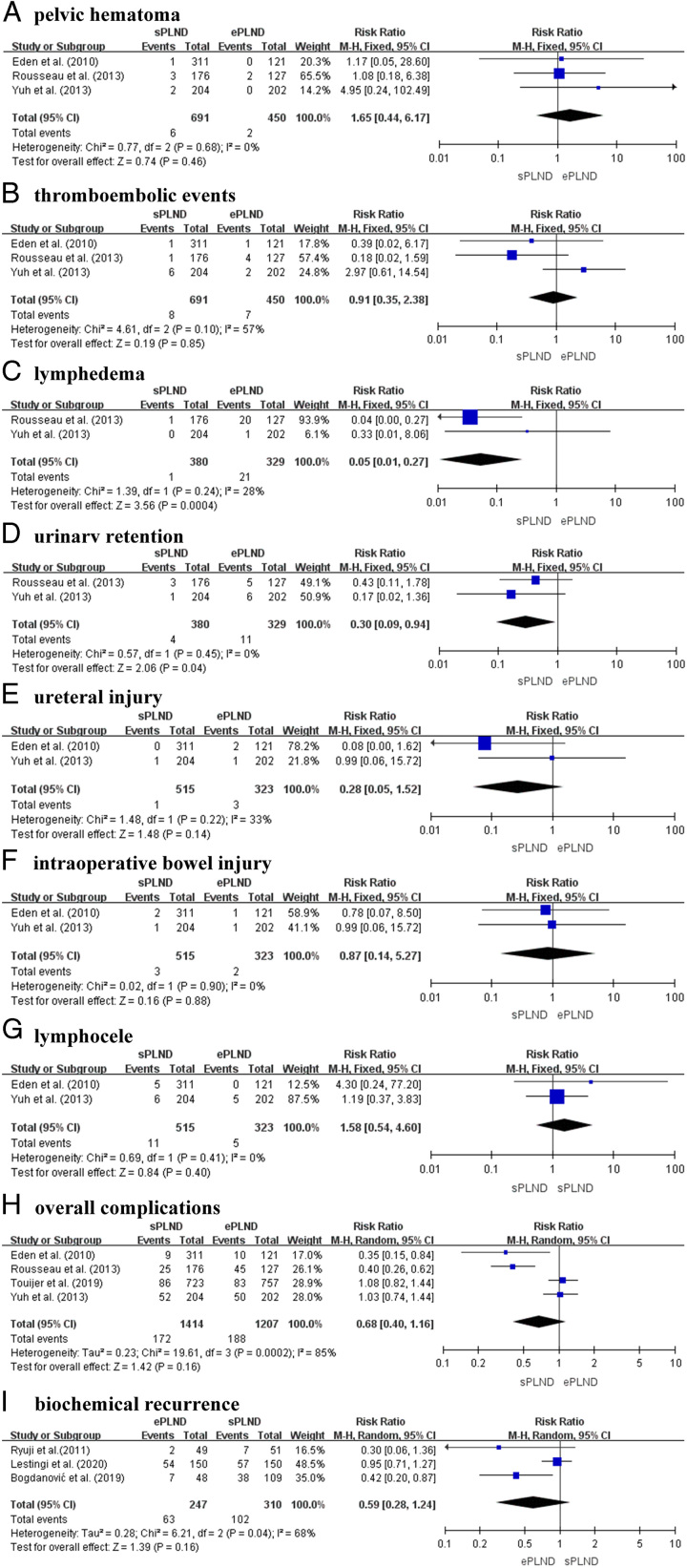
Results: Nine studies, including three randomized clinical trial and six prospective studies, with a total of 4962 patients were analyzed. The meta-analysis revealed that patients undergoing ePLND had a higher risk of partial perioperative complications, such as lymphedema ( I2 =28%; RR 0.05; 95% CI: 0.01-0.27; P <0.001) and urinary retention ( I2 =0%; RR 0.30; 95% CI: 0.09-0.94; P =0.04) compared to those undergoing sPLND. However, there were no significant difference was observed in pelvic hematoma ( I2 =0%; RR 1.65; 95% CI: 0.44-6.17; P =0.46), thromboembolic ( I2 =57%; RR 0.91; 95% CI: 0.35-2.38; P =0.85), ureteral injury ( I2 =33%; RR 0.28; 95% CI: 0.05-1.52; P =0.14), intraoperative bowel injury ( I2 =0%; RR 0.87; 95% CI: 0.14-5.27; P =0.88), and lymphocele ( I2 =0%; RR 1.58; 95% CI: 0.54-4.60; P =0.40) between sPLND and ePLND. Additionally, no significant difference was observed in overall perioperative complications ( I2 =85%; RR 0.68; 95% CI: 0.40-1.16; P =0.16). Furthermore, ePLND did not significantly reduce biochemical recurrence ( I2 =68%; RR 0.59; 95% CI: 0.28-1.24; P =0.16) of prostate cancer.
Conclusion: This analysis found no significant differences in overall perioperative complications or biochemical recurrence between sPLND and ePLND, but ePLND may offer enhanced diagnostic advantages by increasing the detection rate of lymph node metastasis.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare no conflicts of interest.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures
References
-
- Hyndman ME, Mullins JK, Pavlovich CP. Pelvic node dissection in prostate cancer: extended, limited, or not at all? Curr Opin Urol 2010;20:211–217. - PubMed
-
- Palapattu GS, Singer EA, Messing EM. Controversies surrounding lymph node dissection for prostate cancer. Urol Clin North Am 2010;37:57–65; Table of Contents. - PubMed
-
- Briganti A, Blute ML, Eastham JH, et al. . Pelvic lymph node dissection in prostate cancer. Eur Urol 2009;55:1251–1265. - PubMed
-
- Fossati N, Willemse PPM, Van den Broeck T, et al. . The benefits and harms of different extents of lymph node dissection during radical prostatectomy for prostate cancer: a systematic review. Eur Urol 2017;72:84–109. - PubMed
-
- Mohler JL, Armstrong AJ, Bahnson RR, et al. . Prostate Cancer, Version 1.2016. J Natl Compr Canc Netw 2016;14:19–30. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
