

Riding high: seroprevalence of SARS-CoV-2 after 4 pandemic waves in Manitoba, Canada, April 2020-February 2022
- PMID: 38053033
- PMCID: PMC10696886
- DOI: 10.1186/s12889-023-17239-6
Riding high: seroprevalence of SARS-CoV-2 after 4 pandemic waves in Manitoba, Canada, April 2020-February 2022
Abstract
Background: Canada is emerging from the largest SARS-CoV-2 Omicron wave to date, with over 3.3 million confirmed cases. Unfortunately, PCR confirmed cases illuminate only a small portion of infections in the community and underestimate true disease burden. Population based seroprevalence studies, which measure antibody levels against a virus can more accurately estimate infection rates in the community and identify geographical and epidemiological trends to inform public health responses.
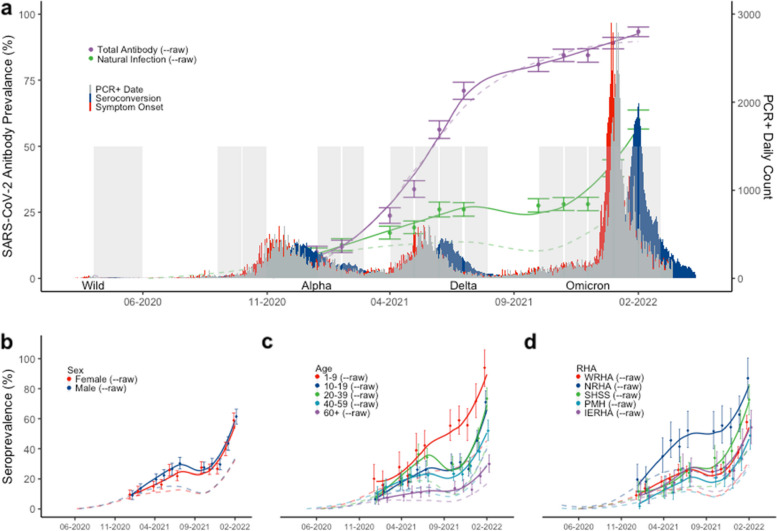
Methods: The Manitoba COVID-19 Seroprevalence (MCS) study is a population-based cross-sectional study to assess the prevalence of SARS-CoV-2 antibodies across the province. Residual convenience specimens (n = 14,901) were tested for anti-SARS-CoV-2 nucleocapsid and spike IgG antibodies from April 1, 2020 to February 31, 2022. We estimated the monthly and cumulative prevalence using an exponential decay model, accounting for population demographics, sensitivity/specificity, and antibody waning. This approach generated estimates of natural infection as well as total antibody including vaccine-induced immunity within the community.
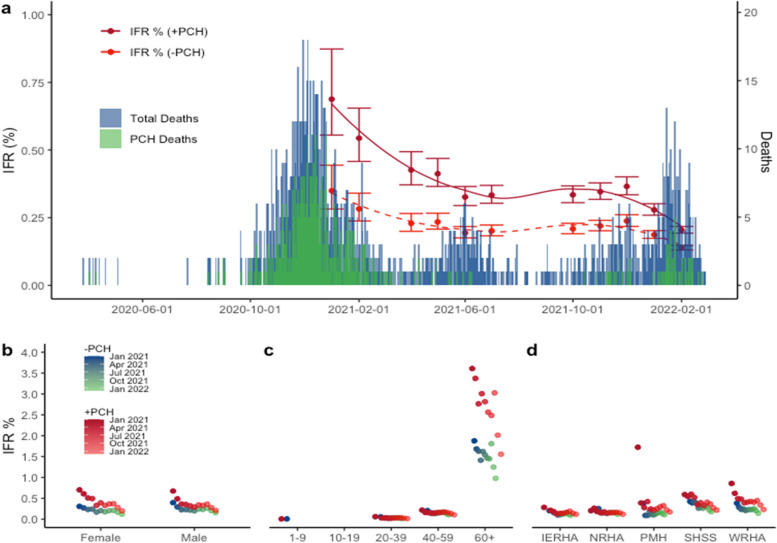
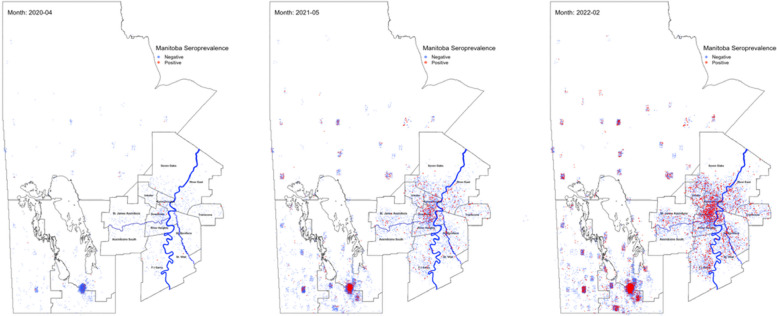
Findings: After four waves of the pandemic, 60.1% (95%CI-56.6-63.7) of Manitobans have generated SARS-CoV-2 antibodies due to natural exposure independent of vaccination. Geographical analysis indicates a large portion of provincial prevalence stems from increased transmission in the Northern (92.3%) and Southern (71.8%) regional health authorities. Despite the high mortality rates reported by Manitoba, infection fatality ratios (IFR) peaked at 0.67% and declined to 0.20% following the Omicron wave, indicating parity with other national and international jurisdictions. Manitoba has achieved 93.4% (95%CI- 91.5-95.1) total antibody when including vaccination.
Interpretation: Our data shows that more than 3 in 5 Manitobans have been infected by SARS-CoV-2 after four waves of the pandemic. This study also identifies key geographical and age specific prevalence rates that have contributed greatly to the overall severity of the pandemic in Manitoba and will inform jurisdictions considering reduction of public health measures.
Keywords: SARS-CoV-2; Serology; Seroprevalence; Vaccination.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Canada S. Impacts of COVID-19 on Canadians – Testingand Vaccination, February 21 toMarch 13, 2022. 2022.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
