

A rare case of full recovery following delayed presentation of paraplegia secondary to thoracic epidural abscess: A case report and review of the literature
- PMID: 38053716
- PMCID: PMC10695466
- DOI: 10.25259/SNI_736_2023
A rare case of full recovery following delayed presentation of paraplegia secondary to thoracic epidural abscess: A case report and review of the literature
Abstract
Background: Timely diagnosis and prompt management of thoracic epidural abscesses are vital to preventing the onset of irreversible paralysis and death.
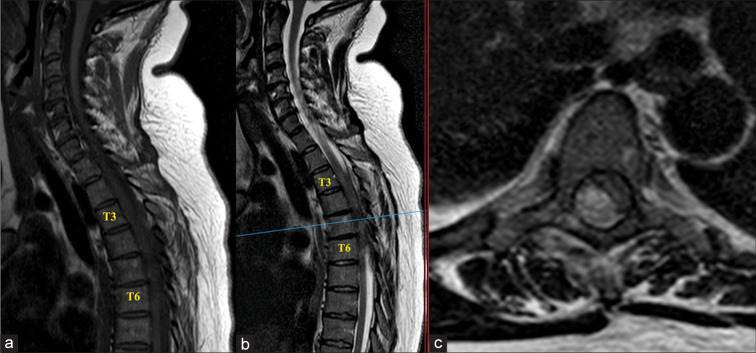
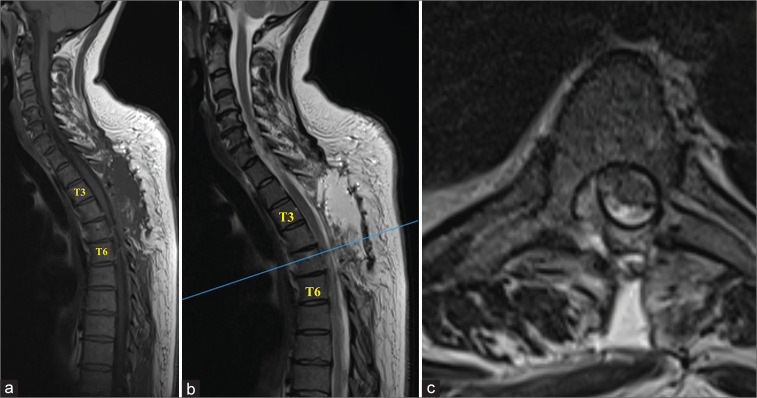
Case description: A 39-year-old female was managed initially for non-specific chest pain for 10 days (i.e., diagnosis of respiratory tract infection). After she developed paraplegia (0/5 motor function), a T10 sensory level, and acute urinary retention, a thoracic magnetic resonance with contrast revealed a T3-T7 spinal epidural abscess with cord compression. On review of her lab studies revealed a white blood cell count of 11.03 × 109/L and a C-reactive protein level of 122 mg/dL. Following a T3-T7 laminectomy with evacuation of an extradural empyema, she fully recovered.
Conclusion: This case report emphasizes the need for early recognition, diagnosis, and treatment of thoracic epidural abscesses that are too often mis-diagnosed as respiratory infections.
Keywords: ASIA A; Delayed presentation of thoracic epidural abscess; Thoracic Laminectomy.
Copyright: © 2023 Surgical Neurology International.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
Epidural abscess as a delayed complication of spinal instrumentation in scoliosis surgery: a case of progressive neurologic dysfunction with complete recovery.Spine (Phila Pa 1976). 2008 Feb 1;33(3):E76-80. doi: 10.1097/BRS.0b013e31816245a6. Spine (Phila Pa 1976). 2008. PMID: 18303449
-
Complete Spinal Cord Injury Secondary to Serratia marcescens Spinal Epidural Abscess: A Report of Significant Neurological Improvement After a Delayed Presentation.Cureus. 2023 Aug 31;15(8):e44451. doi: 10.7759/cureus.44451. eCollection 2023 Aug. Cureus. 2023. PMID: 37791159 Free PMC article.
-
Abdominal pain from a thoracic epidural abscess.J Gen Intern Med. 2006 Feb;21(2):C8-10. doi: 10.1111/j.1525-1497.2005.00259.x. J Gen Intern Med. 2006. PMID: 16606376 Free PMC article.
-
Spontaneous spinal epidural abscess in a neonate. With a review of the literature.Childs Nerv Syst. 2001 Oct;17(10):629-31. doi: 10.1007/s003810100477. Childs Nerv Syst. 2001. PMID: 11685529 Review.
-
Sudden paraplegia due to spontaneous bleeding in a thoracic epidural angiolipoma and literature review.Neurochirurgie. 2018 Mar;64(1):73-75. doi: 10.1016/j.neuchi.2017.08.003. Epub 2018 Feb 19. Neurochirurgie. 2018. PMID: 29472020 Review.
References
-
- Bhise V, Meyer AN, Singh H, Wei L, Russo E, Al-Mutairi A, et al. Errors in diagnosis of spinal epidural abscesses in the era of electronic health records. Am J Med. 2017;130:975–81. - PubMed
-
- Connor DE, Chittiboina P, Caldito G, Nanda A. Comparison of operative and nonoperative management of spinal epidural abscess: A retrospective review of clinical and laboratory predictors of neurological outcome. J Neurosurg Spine. 2013;19:119–127. - PubMed
-
- Reihsaus E, Waldbaur H, Seeling W. Spinal epidural abscess: A meta-analysis of 915 patients. Neurosurg Rev. 2000;23:175–204. - PubMed
-
- Singleton J, Edlow JA. Acute nontraumatic back pain: Risk stratification, emergency department management, and review of serious pathologies. Emerg Med Clin North Am. 2016;34:743–57. - PubMed
-
- Turgut M. Complete recovery of acute paraplegia due to pyogenic thoracic spondylodiscitis with an epidural abscess. Acta Neurochir (Wien) 2008;150:381–6. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous