

Targeting complement in IgA nephropathy
- PMID: 38053977
- PMCID: PMC10695513
- DOI: 10.1093/ckj/sfad198
Targeting complement in IgA nephropathy
Abstract
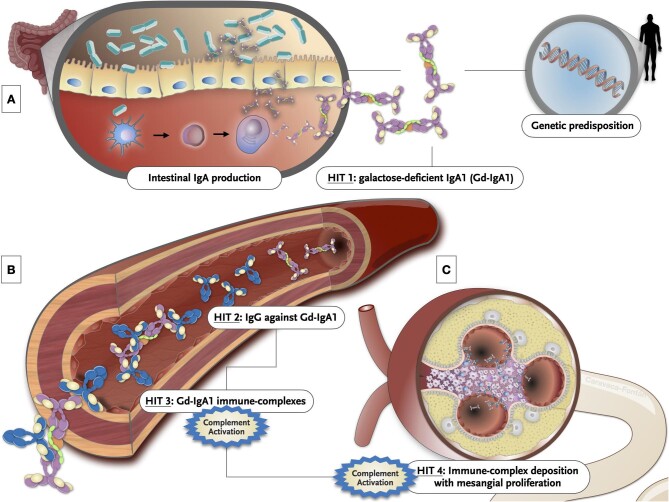
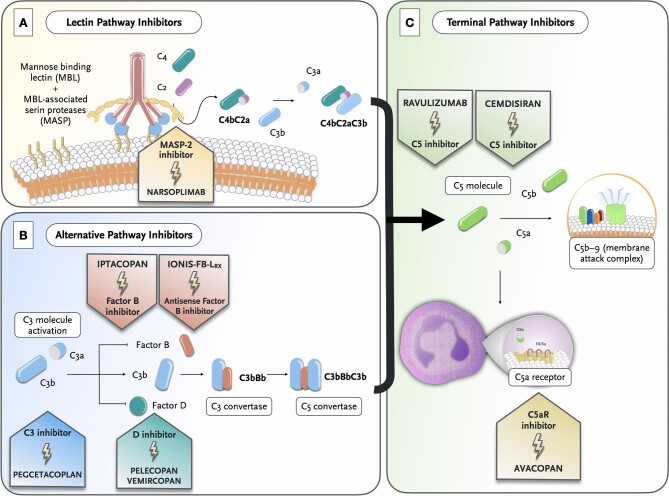
Immunoglobulin A nephropathy (IgAN) is the most common primary glomerulonephritis worldwide. Recent years have witnessed significant improvements in the understanding of the pathogenesis of IgAN and particularly, the pathogenic role of complement activation. The alternative complement pathway is the major complement cascade activator in IgAN, and glomerular C3 deposition has been shown to correlate with disease progression. In addition, several studies have provided insight into the pathogenic role of factor H-related proteins -1 and -5 in IgAN, as independent players in complement dysregulation. The lectin pathway has also been shown to be associated with the severity of IgAN. Glomerular deposition of C4d has been associated with increased histologic disease activity, faster decline in estimated glomerular filtration rate and higher risk of kidney failure. On the other hand, although overlooked in the Oxford classification, numerous studies have shown that the coexistence of thrombotic microangiopathy in IgAN is a significant indicator of a poorer prognosis. All the breakthroughs in the understanding of the contributing role of complement in IgAN have paved the way for the development of new complement-targeted therapies in this disease. Several ongoing trials are evaluating the efficacy of new agents against factor B (iptacopan, Ionis-FB-LRX), C3 (pegcetacoplan), factor D (vemircopan, pelecopan), C5 (ravulizumab, cemdisiran) and C5a receptor 1 (avacopan). In this study, we provide a comprehensive review of the role of complement in IgAN, including the emerging mechanisms of complement activation and the promising potential of complement inhibitors as a viable treatment option for IgAN.
Keywords: IgA nephropathy; alternative pathway; lectin pathway; thrombotic microangiopathy.
© The Author(s) 2023. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
None declared.
Figures

References
-
- Berger J, Hinglais N. Intercapillary deposits of IgA-IgG. J Urol Nephrol (Paris) 1968;74:694–5. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
