

Influence of cardiometabolic medications on abdominal aortic aneurysm growth in the UK Aneurysm Growth Study: metformin and angiotensin-converting enzyme inhibitors associated with slower aneurysm growth
- PMID: 38055889
- PMCID: PMC10763526
- DOI: 10.1093/bjs/znad375
Influence of cardiometabolic medications on abdominal aortic aneurysm growth in the UK Aneurysm Growth Study: metformin and angiotensin-converting enzyme inhibitors associated with slower aneurysm growth
Abstract
Background: There is a clinical need for treatments that can slow or prevent the growth of an abdominal aortic aneurysm, not only to reduce the need for surgery, but to provide a means to treat those who cannot undergo surgery.
Methods: Analysis of the UK Aneurysm Growth Study (UKAGS) prospective cohort was conducted to test for an association between cardiometabolic medications and the growth of an abdominal aortic aneurysm above 30 mm in diameter, using linear mixed-effect models.
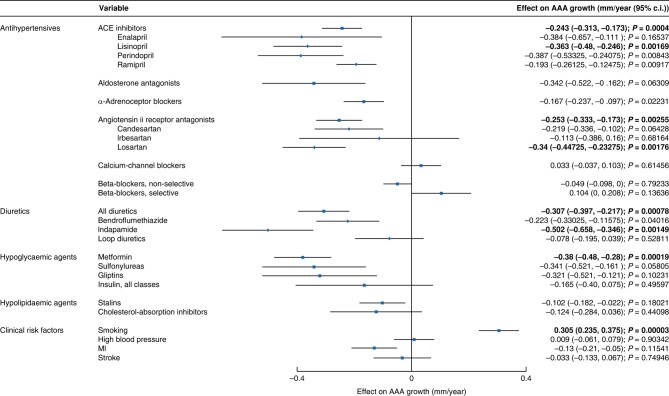
Results: A total of 3670 male participants with data available on abdominal aortic aneurysm growth, smoking status, co-morbidities, and medication history were included. The mean age at recruitment was 69.5 years, the median number of surveillance scans was 6, and the mean(s.e.) unadjusted abdominal aortic aneurysm growth rate was 1.75(0.03) mm/year. In a multivariate linear mixed-effect model, smoking (mean(s.e.) +0.305(0.07) mm/year, P = 0.00003) and antiplatelet use (mean(s.e.) +0.235(0.06) mm/year, P = 0.00018) were found to be associated with more rapid abdominal aortic aneurysm growth, whilst metformin was strongly associated with slower abdominal aortic aneurysm growth (mean(s.e.) -0.38(0.1) mm/year, P = 0.00019), as were angiotensin-converting enzyme inhibitors (mean(s.e.) -0.243(0.07) mm/year, P = 0.0004), angiotensin II receptor antagonists (mean(s.e.) -0.253(0.08) mm/year, P = 0.00255), and thiazides/related diuretics (mean(s.e.) -0.307(0.09) mm/year, P = 0.00078).
Conclusion: The strong association of metformin with slower abdominal aortic aneurysm growth highlights the importance of the ongoing clinical trials assessing the effectiveness of metformin with regard to the prevention of abdominal aortic aneurysm growth and/or rupture. The association of angiotensin-converting enzyme inhibitors, angiotensin II receptor antagonists, and diuretics with slower abdominal aortic aneurysm growth points to the possibility that optimization of cardiovascular risk management as part of abdominal aortic aneurysm surveillance may have the secondary benefit of also reducing abdominal aortic aneurysm growth rates.
© The Author(s) 2023. Published by Oxford University Press on behalf of BJS Society Ltd.
Figures
Comment in
-
Comment on: Influence of cardiometabolic medications on abdominal aortic aneurysm growth in the UK Aneurysm Growth Study: metformin and angiotensin-converting enzyme inhibitors associated with slower aneurysm growth.Br J Surg. 2024 Jul 2;111(7):znae154. doi: 10.1093/bjs/znae154. Br J Surg. 2024. PMID: 38953710 No abstract available.
References
-
- Meecham L, Jacomelli J, Davis M, Pherwani A, Lees T, Earnshaw JJ. Outcomes in men from the NHS Abdominal Aortic Aneurysm Screening Programme with a large aneurysm referred for intervention. Eur J Vasc Endovasc Surg 2021;61:192–199 - PubMed
-
- Jacomelli J, Summers L, Stevenson A, Lees T, Earnshaw JJ. Impact of the first 5 years of a national abdominal aortic aneurysm screening programme. Br J Surg 2016;103:1125–1131 - PubMed
-
- MacSweeney ST, Ellis M, Worrell PC, Greenhalgh RM, Powell JT. Smoking and growth rate of small abdominal aortic aneurysms. Lancet 1994;344:651–652 - PubMed
-
- Sweeting MJ, Thompson SG, Brown LC, Powell JT. Meta-analysis of individual patient data to examine factors affecting growth and rupture of small abdominal aortic aneurysms. Br J Surg 2012;99:655–665 - PubMed
-
- Golledge J, Moxon JV, Singh TP, Bown MJ, Mani K, Wanhainen A. Lack of an effective drug therapy for abdominal aortic aneurysm. J Intern Med 2020;288:6–22 - PubMed
