

Association of blood pressure with neurologic outcome at hospital discharge after pediatric cardiac arrest resuscitation
- PMID: 38056760
- PMCID: PMC11024592
- DOI: 10.1016/j.resuscitation.2023.110066
Association of blood pressure with neurologic outcome at hospital discharge after pediatric cardiac arrest resuscitation
Abstract
Background: Poor outcomes are associated with post cardiac arrest blood pressures <5th percentile for age. We aimed to study the relationship of mean arterial pressure (MAP) with favorable neurologic outcome following cardiac arrest and return of spontaneous circulation (ROSC).
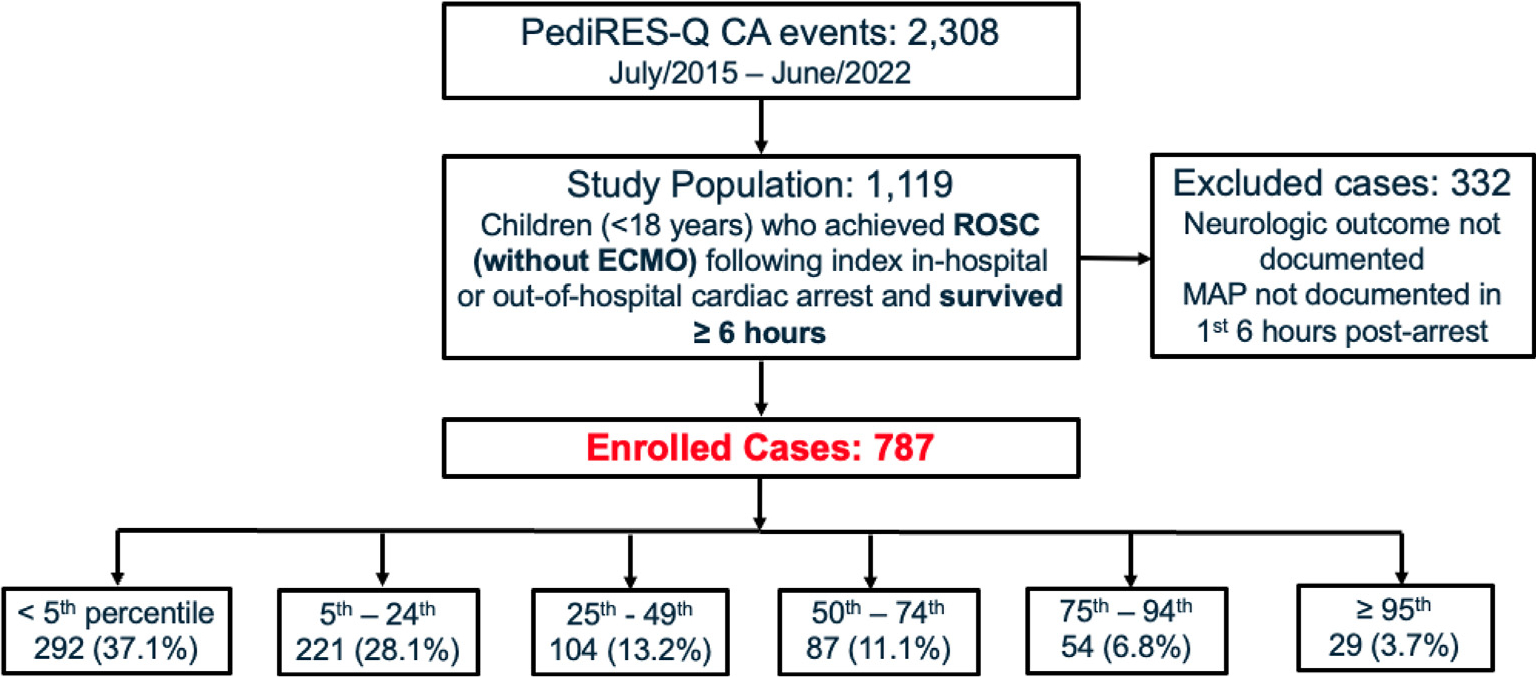
Methods: This retrospective, multi-center, observational study analyzed data from the Pediatric Resuscitation Quality Collaborative (pediRES-Q). Children (<18 years) who achieved ROSC following index in-hospital or out-of-hospital cardiac arrest and survived ≥6 hours were included. Lowest documented MAP within the first 6 hours of ROSC was percentile adjusted for age and categorized into six groups - Group I: <5th, II: 5-24th, III: 25-49th, IV: 50-74th, V: 75-94th; and VI: 95-100th percentile. Primary outcome was favorable neurologic status at hospital discharge, defined as PCPC score 1, 2, or no change from pre-arrest baseline. Multivariable logistic regression was performed to analyze the association of MAP group with favorable outcome, controlling for illness category (surgical-cardiac), initial rhythm (shockable), arrest time (weekend or overnight), age, CPR duration, and clustering by site.
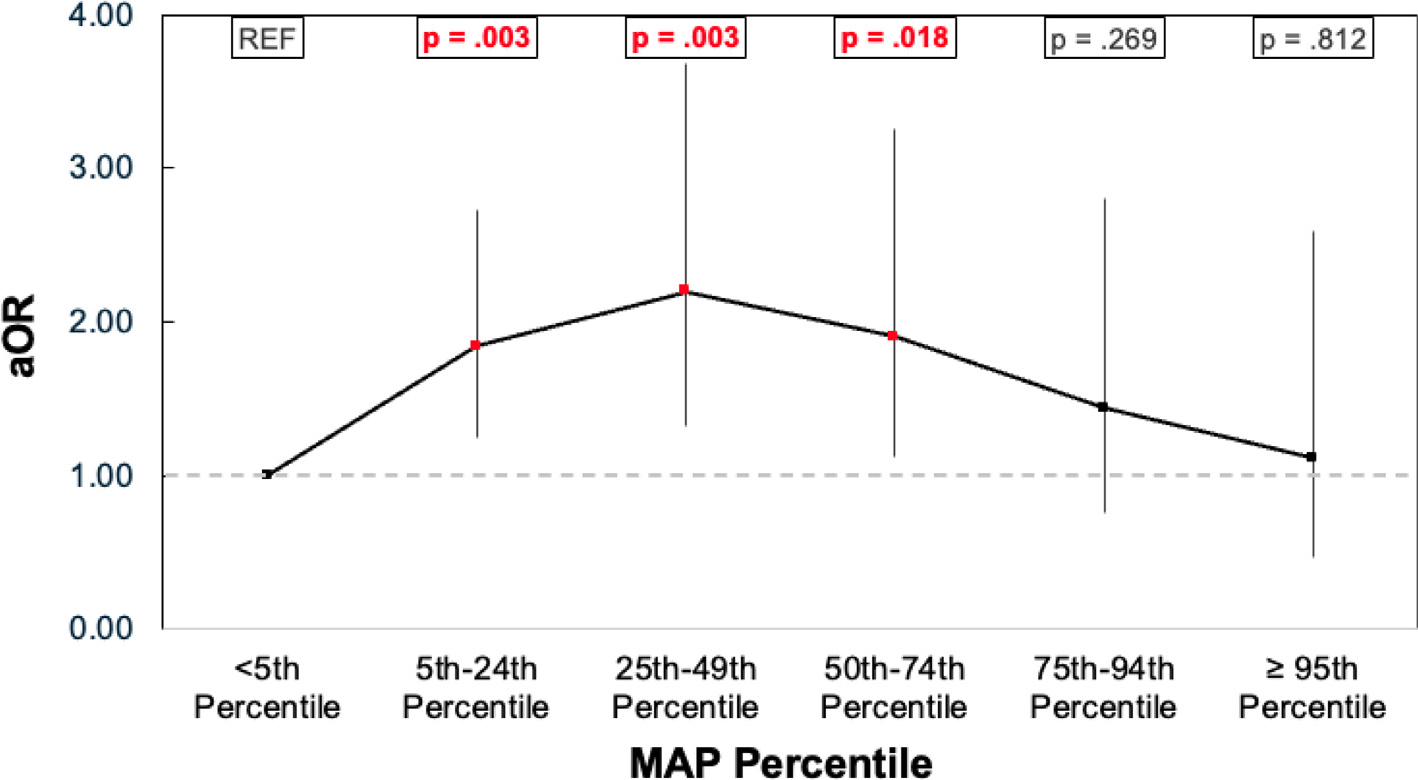
Results: 787 patients were included: median [Q1,Q3] age 17.9 [4.8,90.6] months; male 58%; OHCA 21%; shockable rhythm 13%; CPR duration 7 [3,16] min; favorable neurologic outcome 54%. Median lowest documented MAP percentile for the favorable outcome group was 13 [3,43] versus 8 [1,37] for the unfavorable group. The distribution of blood pressures by MAP group was I: 37%, II: 28%, III: 13%, IV: 11%, V: 7%, and VI: 4%. Compared with patients in Group I (<5%ile), Groups II, III, and IV had higher odds of favorable outcome (aOR, 1.84 [95% CI, 1.24, 2.73]; 2.20 [95% CI, 1.32, 3.68]; 1.90 [95% CI, 1.12, 3.25]). There was no association between Groups V or VI and favorable outcome (aOR, 1.44 [95% CI, 0.75, 2.80]; 1.11 [95% CI, 0.47, 2.59]).
Conclusion: In the first 6-hours post-ROSC, a lowest documented MAP between the 5th-74th percentile for age was associated with favorable neurologic outcome compared to MAP <5th percentile for age.
Keywords: Blood pressure; Cardiopulmonary resuscitation; Hypotension; Outcomes; Pediatrics; Post-cardiac arrest.
Copyright © 2023 Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: The authors declared no financial conflicts of interest. (1) Dana Niles disclosed that the Children’s Hospital of Philadelphia receives support from an unrestricted research grant from ZOLL Medical Corporation. The remaining authors have no disclosures to report. (2) Matthew Kirschen received NIH funding to his institution. (3) Vinay Nadkarni MD received unrestricted research funding to his institution form the National Institutes of Health, Agency for Healthcare Research and Quality, Zoll Medical, Nihon-Kohden Inc., and Volunteers on Scientific Advisory Committees for the American heart Association, Citizen CPR Foundation, INSPIRE simulation network, and Citizen CPR. Dr. Nadkarni is a member of Resuscitation’s Editorial Board. Dr. Nadkarni is the President of the Society of Critical Care Medicine 2022 to 2023. The content reflects his own personal work and is not intended to represent the views of the Society of Critical Care Medicine.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
