

Endovascular thrombectomy for basilar-artery occlusion: A meta-analysis with trial sequential analysis
- PMID: 38058444
- PMCID: PMC10696253
- DOI: 10.1016/j.heliyon.2023.e22953
Endovascular thrombectomy for basilar-artery occlusion: A meta-analysis with trial sequential analysis
Abstract
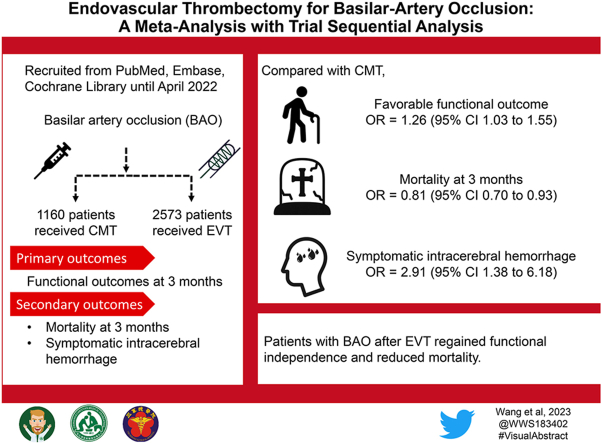
Background and purpose: Basilar-artery occlusion (BAO) usually accounts for devastating neurologic sequelae, poor prognosis, and even death. While endovascular thrombectomy (EVT) is the most successful treatment for anterior circulation stroke with large vessel occlusion, its effectiveness in treating acute BAO is still debatable. Our aim is to compare the efficacy and safety between EVT and conservative medical treatment (CMT) in BAO.
Methods: Up until May 2022, relevant literature was gathered using searches in Embase, PubMed, and the Cochrane Library. The primary outcomes were defined as good functional outcome (modified Rankin Scale 0-2) and favorable functional outcome (modified Rankin Scale 0-3) at 3 months between EVT and CMT groups. The secondary outcomes included mortality at 3 months, symptomatic intracerebral hemorrhage (ICH), and any ICH.
Results: Eight studies involving 3733 patients with BAO were enrolled 2573 individuals underwent EVT, and the remaining 1160 patients received CMT. Compared with CMT, EVT achieved more favorable functional outcome (odds ratio (OR) 1.26, 95% CI 1.03-1.55, I2 = 54%, p = 0.05) in BAO. The good functional outcome showed a similar tendency (OR 1.23, 95% CI 0.97-1.57, I2 = 63%, p = 0.02) as well. EVT decreased mortality at 3 months (OR 0.81, 95% CI 0.70-0.93, I2 = 31 %, p = 0.19), although having a tendency to cause symptomatic ICH (OR 2.91, 95% CI 1.38-6.18, I2 = 22 %, p = 0.27).
Conclusions: EVT in BAO provides superior functional outcomes and less mortality compared with CMT. Even though EVT has the propensity to cause symptomatic ICH, EVT nevertheless improved posterior circulation stroke.
Keywords: Acute ischemic stroke; Basilar-artery occlusion; Endovascular thrombectomy; Meta-analysis.
© 2023 The Authors.
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: This study was supported by the Tri-Service General Hospital/National Defense Medical Center (No. TSGH-D-112157).
Figures



References
-
- Berkhemer O.A., et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N. Engl. J. Med. 2015;372(1):11–20. - PubMed
-
- Goyal M., et al. Randomized assessment of rapid endovascular treatment of ischemic stroke. N. Engl. J. Med. 2015;372(11):1019–1030. - PubMed
-
- Campbell B.C., et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N. Engl. J. Med. 2015;372(11):1009–1018. - PubMed
-
- Saver J.L., et al. Solitaire with the Intention for Thrombectomy as Primary Endovascular Treatment for Acute Ischemic Stroke (SWIFT PRIME) trial: protocol for a randomized, controlled, multicenter study comparing the Solitaire revascularization device with IV tPA with IV tPA alone in acute ischemic stroke. Int. J. Stroke. 2015;10(3):439–448. - PMC - PubMed
-
- Jovin T.G., et al. Thrombectomy within 8 hours after symptom onset in ischemic stroke. N. Engl. J. Med. 2015;372(24):2296–2306. - PubMed
LinkOut - more resources
Full Text Sources
