

First-Line Ipatasertib, Atezolizumab, and Taxane Triplet for Metastatic Triple-Negative Breast Cancer: Clinical and Biomarker Results
- PMID: 38060199
- PMCID: PMC10870115
- DOI: 10.1158/1078-0432.CCR-23-2084
First-Line Ipatasertib, Atezolizumab, and Taxane Triplet for Metastatic Triple-Negative Breast Cancer: Clinical and Biomarker Results
Abstract
Purpose: To evaluate a triplet regimen combining immune checkpoint blockade, AKT pathway inhibition, and (nab-) paclitaxel as first-line therapy for locally advanced/metastatic triple-negative breast cancer (mTNBC).
Patients and methods: The single-arm CO40151 phase Ib study (NCT03800836), the single-arm signal-seeking cohort of IPATunity130 (NCT03337724), and the randomized phase III IPATunity170 trial (NCT04177108) enrolled patients with previously untreated mTNBC. Triplet therapy comprised intravenous atezolizumab 840 mg (days 1 and 15), oral ipatasertib 400 mg/day (days 1-21), and intravenous paclitaxel 80 mg/m2 (or nab-paclitaxel 100 mg/m2; days 1, 8, and 15) every 28 days. Exploratory translational research aimed to elucidate mechanisms and molecular markers of sensitivity and resistance.
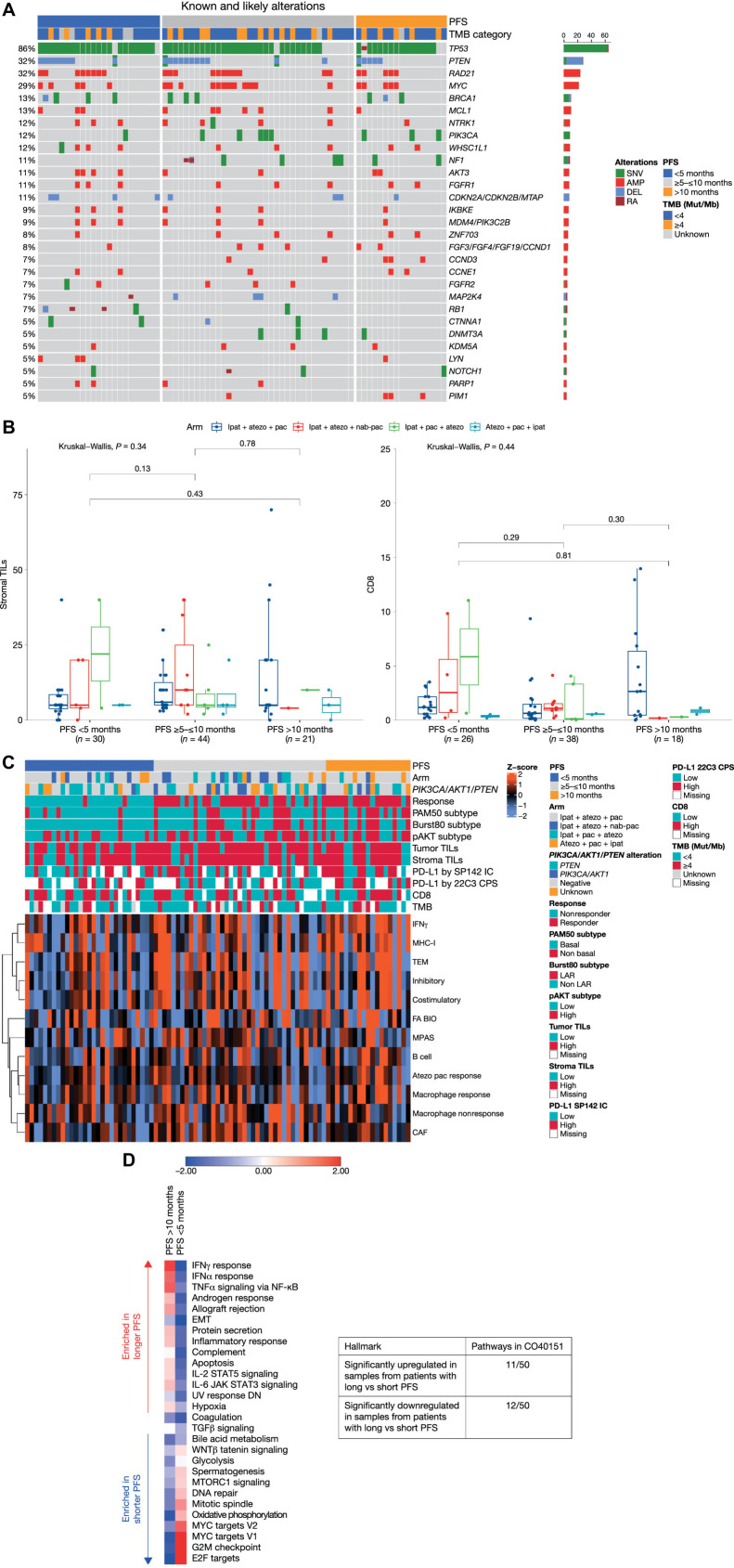
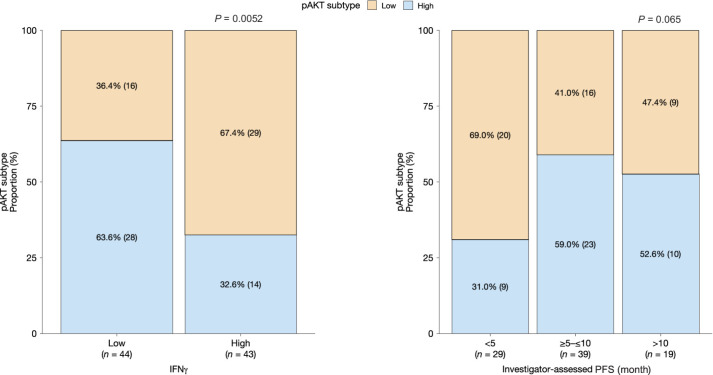
Results: Among 317 patients treated with the triplet, efficacy ranged across studies as follows: median progression-free survival (PFS) 5.4 to 7.4 months, objective response rate 44% to 63%, median duration of response 5.6 to 11.1 months, and median overall survival 15.7 to 28.3 months. The safety profile was consistent with the known toxicities of each agent. Grade ≥3 adverse events were more frequent with the triplet than with doublets or single-agent paclitaxel. Patients with PFS >10 months were characterized by NF1, CCND3, and PIK3CA alterations and increased immune pathway activity. PFS <5 months was associated with CDKN2A/CDKN2B/MTAP alterations and lower predicted phosphorylated AKT-S473 levels.
Conclusions: In patients with mTNBC receiving an ipatasertib/atezolizumab/taxane triplet regimen, molecular characteristics may identify those with particularly favorable or unfavorable outcomes, potentially guiding future research efforts.
©2023 The Authors; Published by the American Association for Cancer Research.
Figures
References
-
- Cortes J, Cescon DW, Rugo HS, Nowecki Z, Im SA, Yusof MM, et al. . Pembrolizumab plus chemotherapy versus placebo plus chemotherapy for previously untreated locally recurrent inoperable or metastatic triple-negative breast cancer (KEYNOTE-355): a randomised, placebo-controlled, double-blind, phase 3 clinical trial. Lancet 2020;396:1817–28. - PubMed
-
- Schmid P, Adams S, Rugo HS, Schneeweiss A, Barrios CH, Iwata H, et al. . Atezolizumab and nab-paclitaxel in advanced triple-negative breast cancer. N Engl J Med 2018;379:2108–21. - PubMed
-
- Emens LA, Adams S, Barrios CH, Diéras V, Iwata H, Loi S, et al. . First-line atezolizumab plus nab-paclitaxel for unresectable, locally advanced, or metastatic triple-negative breast cancer: IMpassion130 final overall survival analysis. Ann Oncol 2021;32:983–93. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
