

Medicaid Insurance is Associated With Decreased MRI Use for Ankle Sprains Compared With Private Insurance: A Retrospective Large-database Analysis
- PMID: 38060239
- PMCID: PMC11272272
- DOI: 10.1097/CORR.0000000000002943
Medicaid Insurance is Associated With Decreased MRI Use for Ankle Sprains Compared With Private Insurance: A Retrospective Large-database Analysis
Abstract
Background: Advanced imaging modalities are expensive, and access to advanced imaging services may vary by socioeconomic factors, creating the potential for unwarranted variations in care. Ankle sprains are a common injury for which variations in MRI use can occur, both via underuse of indicated MRIs (appropriate use) and overuse of nonindicated MRIs (inappropriate use). High-value, equitable healthcare would decrease inappropriate use and increase appropriate use of MRI for this common injury. It is unknown whether socioeconomic factors are associated with underuse of indicated MRIs and overuse of nonindicated MRIs for ankle sprains.
Questions/purposes: Using ankle sprains as a paradigm injury, given their high population incidence, we asked: (1) Does MRI use for ankle sprains vary by insurance type? (2) After controlling for relevant confounding variables, did patients who received an MRI have higher odds of undergoing ankle surgery?
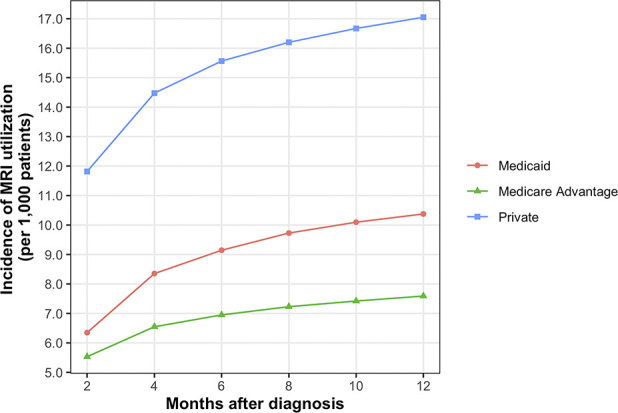
Methods: Between 2011 and 2019, a total of 6,710,223 patients were entered into the PearlDiver Mariner Patient Records Database with a diagnosis of ankle sprain. We considered patients with continuous enrollment in the database for at least 1 year before and 2 years after the diagnosis as potentially eligible. Based on that, 68% (4,567,106) were eligible; a further 20% (1,372,478) were excluded because of age younger than 18 years, age at least 65 years with Medicaid insurance, or age < 65 years with Medicare insurance. Another 0.1% (9169) had incomplete data, leaving 47% (3,185,459) for analysis here. Patients with Medicaid insurance differed from patients with Medicare Advantage or private insurance with respect to age, gender, region, and comorbidity burden. The primary outcome was ankle MRI occurring within 12 months after diagnosis. The use of ankle surgery after MRI in each cohort was measured as a secondary outcome. We used multivariable logistic regression models to evaluate the association between insurance type and MRI use while adjusting for age, gender, region, and comorbidity burden. Separate multivariable regression models were created to evaluate the association between receiving an MRI and subsequent ankle surgery for each insurance type, adjusting for age, gender, region, and comorbidity burden. Within 12 months of an ankle sprain diagnosis, 1% (3522 of 339,457) of patients with Medicaid, 2% (44,793 of 2,627,288) of patients with private insurance, and 1% (1660 of 218,714) of patients with Medicare Advantage received an MRI.
Results: After controlling for age, gender, region, and comorbidity burden, patients with Medicaid had lower odds of receiving an MRI within 12 months after ankle sprain diagnosis than patients with private insurance (odds ratio 0.60 [95% confidence interval 0.57 to 0.62]; p < 0.001). Patients with Medicaid who received an MRI had higher adjusted odds of undergoing subsequent ankle surgery (OR 23 [95% CI 21 to 26]; p < 0.001) than patients with private insurance (OR 12.7 [95% CI 12 to 13]; p < 0.001).
Conclusion: Although absolute MRI use was generally low, there was substantial relative variation by insurance type. Given the high incidence of ankle sprains in the general population, these relative differences can translate to tens of thousands of MRIs. Further studies are needed to evaluate the reasons for decreased appropriate MRI use in patients with Medicaid and overuse of MRI in patients with private insurance. The establishment of clinical practice guidelines by orthopaedic professional societies and more stringent gatekeeping for MRI use by health insurers could reduce unwarranted variations in MRI use.
Level of evidence: Level III, prognostic study.
Copyright © 2023 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
Each author certifies that there are no funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article related to the author or any immediate family members. All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Figures

Similar articles
-
Does Augmenting Irradiated Autografts With Free Vascularized Fibula Graft in Patients With Bone Loss From a Malignant Tumor Achieve Union, Function, and Complication Rate Comparably to Patients Without Bone Loss and Augmentation When Reconstructing Intercalary Resections in the Lower Extremity?Clin Orthop Relat Res. 2025 Jun 26. doi: 10.1097/CORR.0000000000003599. Online ahead of print. Clin Orthop Relat Res. 2025. PMID: 40569278
-
Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients With Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone.Clin Orthop Relat Res. 2024 Dec 1;482(12):2193-2208. doi: 10.1097/CORR.0000000000003185. Epub 2024 Jul 23. Clin Orthop Relat Res. 2024. PMID: 39051924
-
Sexual Harassment and Prevention Training.2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 36508513 Free Books & Documents.
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.Health Technol Assess. 2008 Jun;12(28):iii-iv, ix-95. doi: 10.3310/hta12280. Health Technol Assess. 2008. PMID: 18547499
-
Physician anaesthetists versus non-physician providers of anaesthesia for surgical patients.Cochrane Database Syst Rev. 2014 Jul 11;2014(7):CD010357. doi: 10.1002/14651858.CD010357.pub2. Cochrane Database Syst Rev. 2014. PMID: 25019298 Free PMC article.
Cited by
-
CORR Insights®: Medicaid Insurance is Associated With Decreased MRI Use for Ankle Sprains Compared With Private Insurance: A Large-database Analysis.Clin Orthop Relat Res. 2024 Aug 1;482(8):1403-1405. doi: 10.1097/CORR.0000000000002981. Epub 2024 Jan 26. Clin Orthop Relat Res. 2024. PMID: 38294278 Free PMC article. No abstract available.
References
-
- Amen TB, Liimakka AP, Jain B, Rudisill SS, Bedair HS, Chen AF. Total joint arthroplasty utilization after orthopaedic surgery referral: identifying disparities along the care pathway. J Arthroplasty. 2023;38:424-430. - PubMed
-
- Baker LC. Acquisition of MRI equipment by doctors drives up imaging use and spending. Health Aff (Millwood). 2010;29:2252-2259. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
