

A Nationwide Comparative Analysis of Temperature-Related Mortality and Morbidity in Japan
- PMID: 38060264
- PMCID: PMC10702932
- DOI: 10.1289/EHP12854
A Nationwide Comparative Analysis of Temperature-Related Mortality and Morbidity in Japan
Abstract
Background: The impact of temperature on morbidity remains largely unknown. Moreover, extensive evidence indicates contrasting patterns between temperature-mortality and temperature-morbidity associations. A nationwide comparison of the impact of temperature on mortality and morbidity in more specific subgroups is necessary to strengthen understanding and help explore underlying mechanisms by identifying susceptible populations.
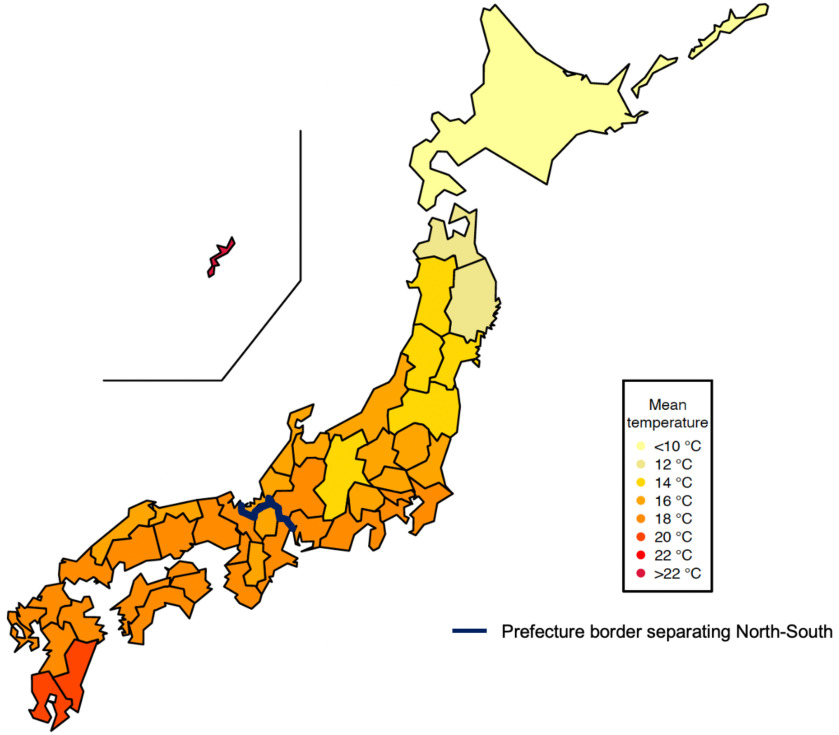
Objective: We performed this study to quantify and compare the impact of temperature on mortality and morbidity in 47 prefectures in Japan.
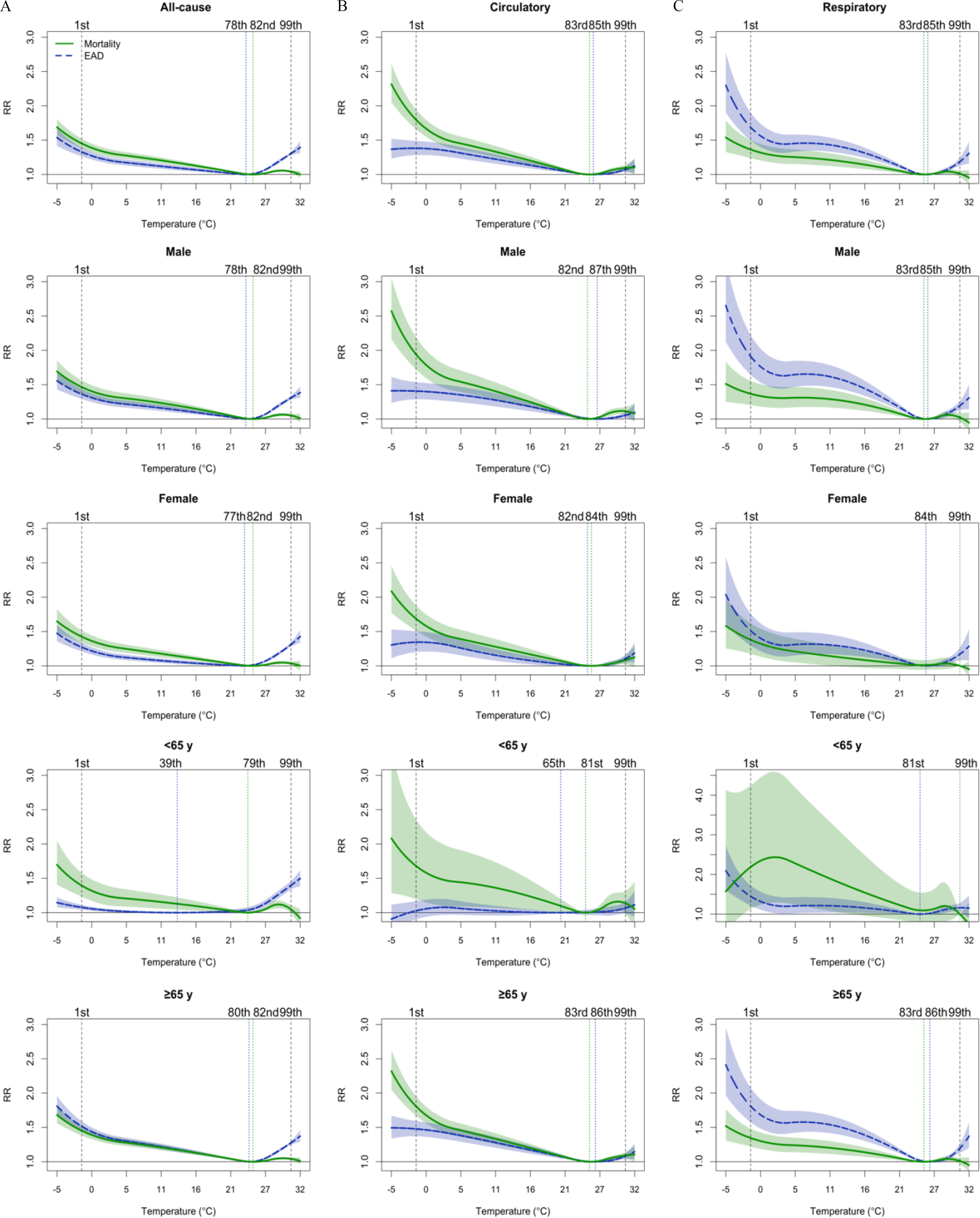
Methods: We applied a two-stage time-series design with distributed lag nonlinear models and mixed-effect multivariate meta-analysis to assess the association of temperature with mortality and morbidity by causes (all-cause, circulatory, and respiratory) at prefecture and country levels between 2015 and 2019. Subgroup analysis was conducted by sex, age, and regions.
Results: The patterns and magnitudes of temperature impacts on morbidity and mortality differed. For all-cause outcomes, cold exhibited larger effects on mortality, and heat showed larger effects on morbidity. At specific temperature percentiles, cold (first percentile) was associated with a higher relative risk (RR) of mortality [1.45; 95% confidence interval (CI): 1.39, 1.52] than morbidity (1.33; 95% CI: 1.26, 1.40), as compared to the minimum mortality/morbidity temperature. Heat (99th percentile) was associated with a higher risk of morbidity (1.30; 95% CI: 1.28, 1.33) than mortality (1.04; 95% CI: 1.02, 1.06). For cause-specific diseases, mortality due to circulatory diseases was more susceptible to heat and cold than morbidity. However, for respiratory diseases, both cold and heat showed higher risks for morbidity than mortality. Subgroup analyses suggested varied associations depending on specific outcomes.
Discussion: Distinct patterns were observed for the association of temperature with mortality and morbidity, underlying different mechanisms of temperature on different end points, and the differences in population susceptibility are possible explanations. Future mitigation policies and preventive measures against nonoptimal temperatures should be specific to disease outcomes and targeted at susceptible populations. https://doi.org/10.1289/EHP12854.
Figures


References
-
- Murray CJL, Aravkin AY, Zheng P, Abbafati C, Abbas KM, Abbasi-Kangevari M, et al. . 2020. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet 396(10258):1223–1249, PMID: , 10.1016/S0140-6736(20)30752-2. - DOI - PMC - PubMed
-
- Bunker A, Wildenhain J, Vandenbergh A, Henschke N, Rocklöv J, Hajat S, et al. . 2016. Effects of air temperature on climate-sensitive mortality and morbidity outcomes in the elderly; a systematic review and meta-analysis of epidemiological evidence. EBioMedicine 6:258–268, PMID: , 10.1016/j.ebiom.2016.02.034. - DOI - PMC - PubMed
-
- Son JY, Liu JC, Bell ML. 2019. Temperature-related mortality: a systematic review and investigation of effect modifiers. Environ Res Lett 14(7):073004, 10.1088/1748-9326/ab1cdb. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
