

Resolving the Dance: A Case Study on Non-Ketotic Hyperglycemic Hemichorea-Hemiballismus in a Patient with Long-Standing Type 2 Diabetes
- PMID: 38064410
- PMCID: PMC10721340
- DOI: 10.12659/AJCR.941443
Resolving the Dance: A Case Study on Non-Ketotic Hyperglycemic Hemichorea-Hemiballismus in a Patient with Long-Standing Type 2 Diabetes
Abstract
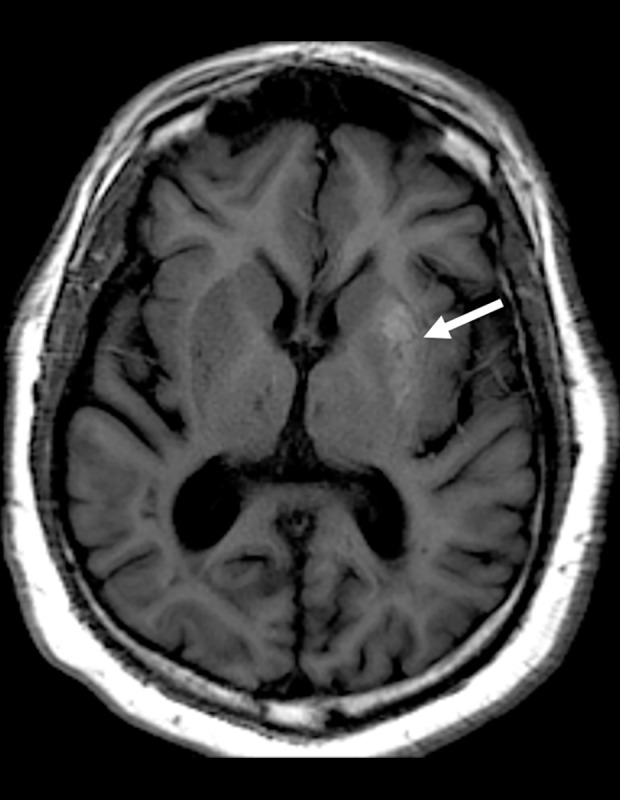
BACKGROUND Non-ketotic hyperglycemic hemichorea-hemiballism (HCHB) is a rare complication of diabetes, which is mainly described in case reports. This condition occurs more commonly in older women and is known to be associated with T1 hyperintensity basal ganglia lesions on magnetic resonance imaging (MRI). The pathophysiology of non-ketotic hyperglycemic HCHB is not well defined, although a combination of regional metabolic failure and ischemia due to hyperglycemia is suspected to occur. Treatment entails tight blood glucose control, although antipsychotic medications such as risperidone may be helpful in refractory cases. CASE REPORT We describe a case of a middle-aged man with long-standing type 2 diabetes who experienced 3 weeks of progressive unilateral arm, leg, and face choreiform movements. Laboratory testing performed just prior to symptom onset was notable for a hemoglobin A1C of >15% and a serum blood glucose of 566 mg/dl. MRI revealed diffuse T1 hyperintensity in the left lentiform nucleus. Our patient's insulin regimen was adjusted, resulting in improvement in average serum glucose (A1C of 9.4%). However, his symptoms did not improve significantly. A trial of benzodiazepine was attempted, without success. When risperidone was started, the patient experienced resolution of symptoms. Recurrence of non-ketotic hyperglycemic HCHB while off risperidone has not occurred to date. CONCLUSIONS Non-ketotic hyperglycemic HCHB is a rare but important diagnosis to consider in patients with hyperglycemia and new-onset choreiform movements. Patients with long-standing type 2 diabetes may be affected, especially when glycemic control worsens. When tight blood glucose control does not resolve symptoms, a short course of antipsychotic agents may provide relief.
Conflict of interest statement
Figures
Similar articles
-
Hemichorea-hemiballismus in non-ketotic hyperglycaemia.J Clin Neurosci. 2011 Feb;18(2):293-4. doi: 10.1016/j.jocn.2010.04.036. Epub 2010 Dec 14. J Clin Neurosci. 2011. PMID: 21159513
-
Hemichorea-hemiballismus due to diabetic striatopathy a serious complication of uncontrolled diabetes.BMJ Case Rep. 2024 May 22;17(5):e259046. doi: 10.1136/bcr-2023-259046. BMJ Case Rep. 2024. PMID: 38782432 Free PMC article.
-
Nonketotic hyperglycemia hemichorea and hemiballismus: a case report.J Med Case Rep. 2024 Mar 12;18(1):154. doi: 10.1186/s13256-023-04332-y. J Med Case Rep. 2024. PMID: 38468351 Free PMC article.
-
[Clinical characteristics of hemichorea associated with non-ketotic hyperglycemia in 3 patients: case report and literature review].Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2017 Nov 28;42(11):1341-1347. doi: 10.11817/j.issn.1672-7347.2017.11.016. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2017. PMID: 29187664 Review. Chinese.
-
Diabetic striatopathy: an updated overview of current knowledge and future perspectives.J Endocrinol Invest. 2024 Jan;47(1):1-15. doi: 10.1007/s40618-023-02166-5. Epub 2023 Aug 14. J Endocrinol Invest. 2024. PMID: 37578646 Free PMC article. Review.
References
-
- Cheema H, Federman D, Kam A. Hemichorea-hemiballismus in non-ketotic hyperglycaemia. J Clin Neurosci. 2011;18:293–94. - PubMed
-
- Ifergane G, Masalha R, Herishanu YO. Transient hemichorea/hemiballismus associated with new onset hyperglycemia. Can J Neurol Sci. 2001;28:365–68. - PubMed
-
- Ryan C, Ahlskog E, Savica R. Hyperglycemia chorea/ballism ascertained over 15 years at a referral medical center. Parkinsonism Relat Disord. 2018;48:97–100. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
