

Reflectance Confocal Microscopy and Dermoscopy of Facial Pigmented and Non-Pigmented Actinic Keratosis Features before and after Photodynamic Therapy Treatment
- PMID: 38067302
- PMCID: PMC10705734
- DOI: 10.3390/cancers15235598
Reflectance Confocal Microscopy and Dermoscopy of Facial Pigmented and Non-Pigmented Actinic Keratosis Features before and after Photodynamic Therapy Treatment
Abstract
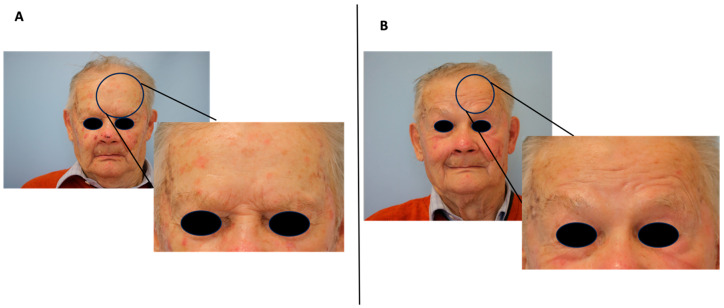
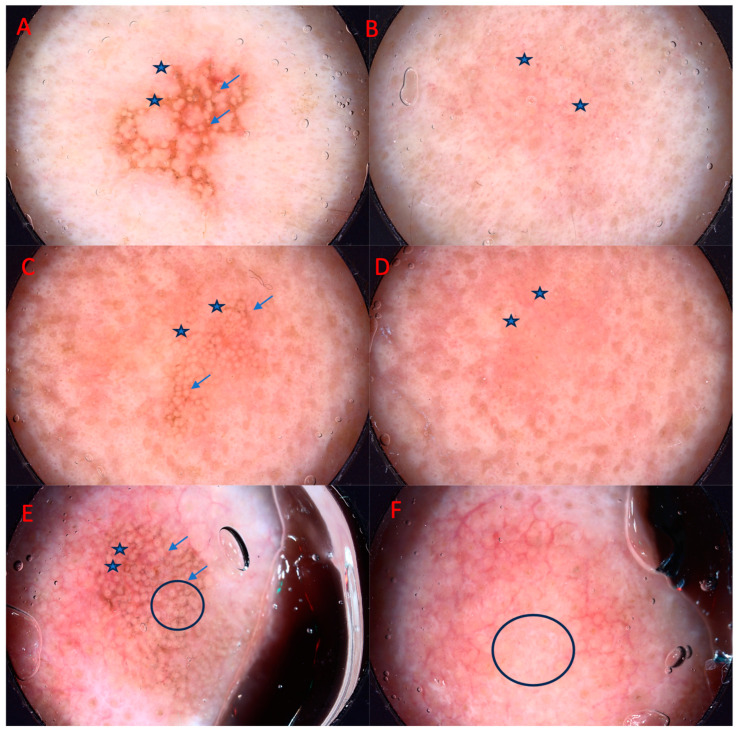
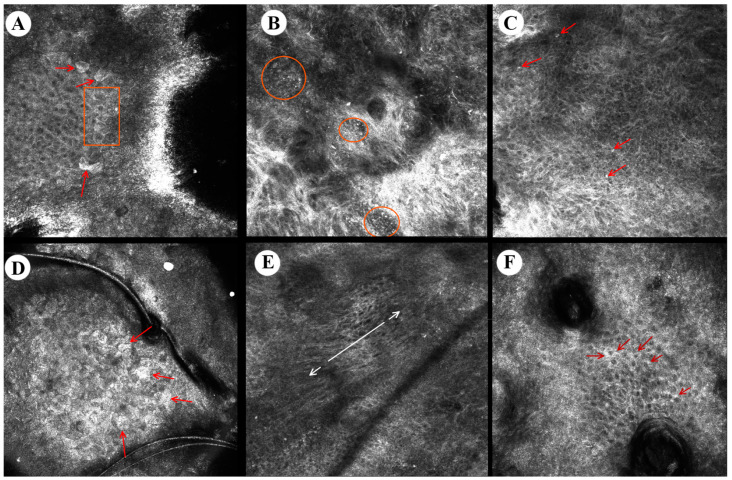
Actinic keratosis (AK), due to its widespread prevalence, as well as the possibility of progression to an invasive form of squamous cell carcinoma, requires treatment regardless of the clinical stage. New imaging techniques, such as in vivo reflectance confocal microscopy (RCM), significantly increase the accuracy of diagnosis and allow noninvasive evaluation of the therapeutic efficacy of the ongoing treatment. Our objective was to evaluate the prevalence of specific (video)dermoscopy and RCM features of pigmented and classical subtypes of AK before and after photodynamic therapy (PDT) treatment. We included patients with facial grade II AKs (25 pigmented, 275 non-pigmented) were included in the study. Skin lesions were evaluated by (video)dermoscopy and RCM at the baseline and three months after PDT. In classic AK, the most frequent dermoscopic findings were fine wavy vessels (96%), scale (92%), microerosions (48%), and "strawberry" pattern (36%), while pigmented AK was characterized mostly by "rhomboidal pattern" (80%), scale (60%), white globules (48%), "jelly sign", and superficial pigmentation (40%). RCM's most characteristic classic AK findings were abnormal honeycomb pattern in the spinous layer, epidermal inflammatory infiltrate, and solar elastosis that were present in 96% of lesions. Pigmented AKs presented mostly with dark central areas of parakeratosis (72%), mottled pigmentation (72%), dermal inflammatory infiltrate (64%), solar elastosis (60%), and abnormal honeycomb pattern in the spinous layer (56%). Dermoscopically, PDT resulted in complete disappearance of the "rhomboidal pattern" in both classical and pigmented AKs, "starburst pattern" and "jelly sign" in classical AKs, and inner gray halo, "rosette sign" and central crust in pigmented AKs. Three months after one PDT session, RCM evaluation showed mostly solar elastosis in both classical and pigmented AK subtypes, epidermal inflammatory infiltrate in classical AKs, and dermal inflammatory infiltrate in pigmented AKs. New noninvasive imaging techniques such as RCM and (video)dermoscopy can help practitioners better visualize the efficacy of the ongoing PDT treatment in either classical or pigmented AK subtypes.
Keywords: AK; PDT; RCM; actinic keratosis; dermoscopy; photodynamic therapy; reflectance confocal microscopy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Role of In Vivo Reflectance Confocal Microscopy in the Analysis of Melanocytic Lesions.Acta Dermatovenerol Croat. 2018 Apr;26(1):64-67. Acta Dermatovenerol Croat. 2018. PMID: 29782304 Review.
-
Photodynamic Therapy is an Effective Treatment of Facial Pigmented Actinic Keratosis.Dermatol Ther (Heidelb). 2023 Jun;13(6):1265-1276. doi: 10.1007/s13555-023-00924-0. Epub 2023 May 10. Dermatol Ther (Heidelb). 2023. PMID: 37162710 Free PMC article.
-
Dermoscopy and reflectance confocal microscopy of pigmented actinic keratoses: a morphological study.J Eur Acad Dermatol Venereol. 2015 Feb;29(2):307-314. doi: 10.1111/jdv.12532. Epub 2014 Apr 22. J Eur Acad Dermatol Venereol. 2015. PMID: 24754497
-
Effects of topical piroxicam and sun filters in actinic keratosis evolution and field cancerization: a two-center, assessor-blinded, clinical, confocal microscopy and dermoscopy evaluation trial.Curr Med Res Opin. 2019 Oct;35(10):1785-1792. doi: 10.1080/03007995.2019.1626227. Epub 2019 Jun 13. Curr Med Res Opin. 2019. PMID: 31148490 Clinical Trial.
-
Dermoscopic features of actinic keratosis.J Dtsch Dermatol Ges. 2007 Nov;5(11):970-6. doi: 10.1111/j.1610-0387.2007.06318.x. Epub 2007 Oct 1. J Dtsch Dermatol Ges. 2007. PMID: 17908179 Review. English, German.
Cited by
-
Vascular feature identification in actinic keratosis grades I-III using dynamic optical coherence tomography with automated, quantitative analysis.Arch Dermatol Res. 2024 Jun 15;316(7):391. doi: 10.1007/s00403-024-03022-z. Arch Dermatol Res. 2024. PMID: 38878217 Free PMC article.
-
An Update on Non-Invasive Skin Imaging Techniques in Actinic Keratosis-A Narrative Review.Medicina (Kaunas). 2024 Jun 26;60(7):1043. doi: 10.3390/medicina60071043. Medicina (Kaunas). 2024. PMID: 39064472 Free PMC article. Review.
-
Vascular Characteristics of Treatment-resistant and -responsive Actinic Keratosis Identified with Dynamic Optical Coherence Tomography.Acta Derm Venereol. 2024 Nov 25;104:adv42190. doi: 10.2340/actadv.v104.42190. Acta Derm Venereol. 2024. PMID: 39585185 Free PMC article.
References
-
- Richard M.A., Amici J.M., Basset-Seguin N., Claudel J.P., Cribier B., Dreno B. Management of actinic keratosis at specific body sites in patients at high risk of carcinoma lesions: Expert consensus from the AKTeam™ of expert clinicians. J. Eur. Acad. Dermatol. Venereol. 2018;32:339–346. doi: 10.1111/jdv.14753. - DOI - PubMed
-
- Ahmady S., Jansen M.H.E., Nelemans P.J., Kessels J., Arits A., de Rooij M.J.M., Essers B.A.B., Quaedvlieg P.J.F., Kelleners-Smeets N.W.J., Mosterd K. Risk of Invasive Cutaneous Squamous Cell Carcinoma after Different Treatments for Actinic Keratosis: A Secondary Analysis of a Randomized Clinical Trial. JAMA Dermatol. 2022;158:634–640. doi: 10.1001/jamadermatol.2022.1034. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
