

Urethral Mesh Assessment in Cancer Patients
- PMID: 38067303
- PMCID: PMC10705124
- DOI: 10.3390/cancers15235599
Urethral Mesh Assessment in Cancer Patients
Abstract
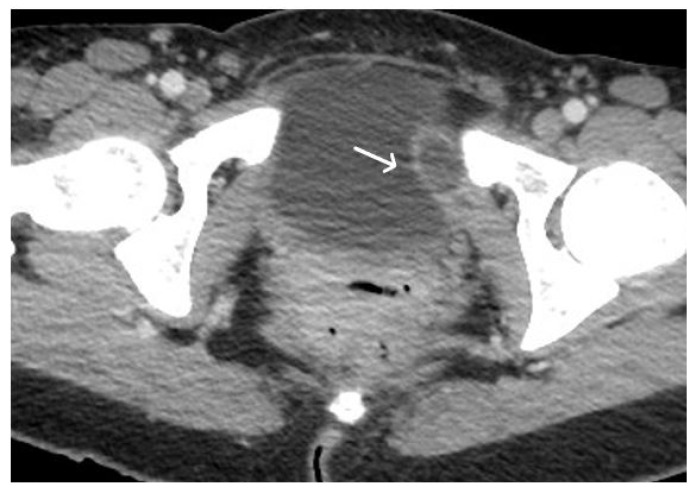
Urethral mesh placement has become a common surgical intervention for the management of stress urinary incontinence. While this procedure offers significant benefits, it is not without potential complications. This review article aims to provide a comprehensive overview of urethral mesh assessment in oncologic patients. The article explores normal magnetic resonance imaging (MRI) and computed tomography (CT) mesh appearances and highlights the pathological aspects associated with urethral mesh complications including both short-term and long-term post-operative complications. By understanding the spectrum of normal findings of urethral mesh and the possible complications, clinicians can improve patient outcomes and make informed decisions regarding urethral mesh management in this patient population.
Keywords: TOT; TVT; mesh; urethral mesh; urethral neoplasm.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


















Similar articles
-
Long-term efficacy and complications of a multicentre randomised controlled trial comparing retropubic and transobturator mid-urethral slings: a prospective observational study.BJOG. 2021 Dec;128(13):2191-2199. doi: 10.1111/1471-0528.16899. Epub 2021 Oct 6. BJOG. 2021. PMID: 34478604 Clinical Trial.
-
Comparison of TVT and TOT on urethral mobility and surgical outcomes in stress urinary incontinence with hypermobile urethra.Eur J Obstet Gynecol Reprod Biol. 2015 Jul;190:36-40. doi: 10.1016/j.ejogrb.2015.04.010. Epub 2015 Apr 30. Eur J Obstet Gynecol Reprod Biol. 2015. PMID: 25966437
-
The Rate of Mesh Erosion after Modified Transobturator Tape (Canal Transobturator Tape) Surgery: Analysis of 5 years' Outcome and Influencing Factors.Urol Int. 2019;103(4):482-487. doi: 10.1159/000503155. Epub 2019 Oct 23. Urol Int. 2019. PMID: 31645045
-
Adductor brevis myositis following transobturator tape procedure: a case report and review of the literature.Int Urogynecol J Pelvic Floor Dysfunct. 2007 Jul;18(7):817-20. doi: 10.1007/s00192-006-0220-9. Epub 2007 Feb 15. Int Urogynecol J Pelvic Floor Dysfunct. 2007. PMID: 17577593 Review.
-
Role of endoscopic management in synthetic sling/mesh erosion following previous incontinence surgery: a systematic review from European Association of Urologists Young Academic Urologists (YAU) and Uro-technology (ESUT) groups.Int Urogynecol J. 2020 Jan;31(1):45-53. doi: 10.1007/s00192-019-04087-5. Epub 2019 Aug 29. Int Urogynecol J. 2020. PMID: 31468095 Free PMC article.
References
-
- Afonso J.S., Jorge R.M., Martins P.S., Soldi Mda S., Alves O.L., Patricio B., Mascarenhas T., Sartori M.G., Girao M.J. Structural and thermal properties of polypropylene mesh used in treatment of stress urinary incontinence. Acta Bioeng. Biomech. 2009;11:27–33. - PubMed
-
- Delorme E. Trans-obturator urethral suspension: A minimally invasive procedure to treat female stress urinary incontinence. Prog. Urol. 2001;11:1306–1313. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
