

Review of Current Treatment Intensification Strategies for Prostate Cancer Patients
- PMID: 38067321
- PMCID: PMC10705205
- DOI: 10.3390/cancers15235615
Review of Current Treatment Intensification Strategies for Prostate Cancer Patients
Abstract
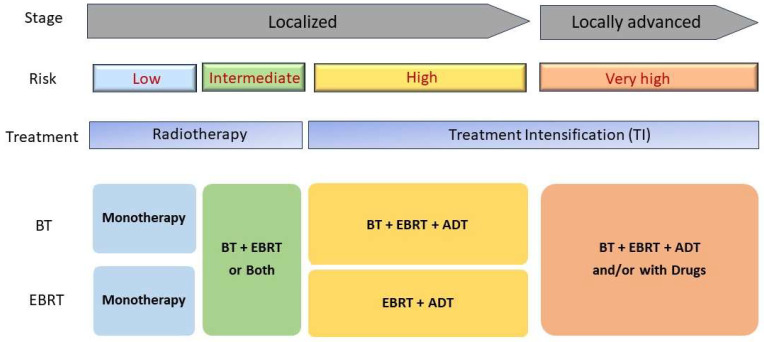
Prostate cancer (PCa) used to be one of the most common nondermatologic cancers in men that can be treated only with surgery. However, a revolutionary breakthrough came in the 1980s with the introduction of long-acting luteinizing hormone-releasing hormone (LHRH) agonists for the curative treatment of PCa. This paradigm shift contributed to the combined use of androgen deprivation therapy (ADT), chemotherapy, and radiotherapy for the treatment. The latest data highlight the use of treatment intensification (TI), i.e., combined use of radiotherapy (RT) and hormonal or drug treatments, for localized or locally advanced PCa. Indeed, the results of combined modality treatments have shown a reduction in disease-specific mortality and improved overall survival. Although TI seems promising, more research studies are warranted to confirm its efficacy. This review summarizes the latest available outcome results of pivotal trials and clinical studies on the efficacy of TI.
Keywords: ADT; LHRH agonist; prostate cancer; radiotherapy/radiation therapy; treatment intensification.
Conflict of interest statement
The authors declare no conflict of interest. The sponsor of the study was not involved in the study design, analysis, and interpretation of data; writing of the report; or the decision to submit the study results for publication.
Figures
Similar articles
-
Benefits and Risks of Primary Treatments for High-risk Localized and Locally Advanced Prostate Cancer: An International Multidisciplinary Systematic Review.Eur Urol. 2020 May;77(5):614-627. doi: 10.1016/j.eururo.2020.01.033. Epub 2020 Mar 4. Eur Urol. 2020. PMID: 32146018
-
Luteinizing hormone-releasing hormone agonists in the treatment of prostate cancer: a review of their discovery, development, and place in therapy.Clin Ther. 2006 Oct;28(10):1485-508. doi: 10.1016/j.clinthera.2006.10.018. Clin Ther. 2006. PMID: 17157109 Review.
-
Agonists of luteinizing hormone-releasing hormone in prostate cancer.Expert Opin Pharmacother. 2013 Nov;14(16):2237-47. doi: 10.1517/14656566.2013.834328. Epub 2013 Aug 28. Expert Opin Pharmacother. 2013. PMID: 23984804 Review.
-
Androgen-deprivation therapy as primary treatment for localized prostate cancer: data from Cancer of the Prostate Strategic Urologic Research Endeavor (CaPSURE).Cancer. 2006 Apr 15;106(8):1708-14. doi: 10.1002/cncr.21799. Cancer. 2006. PMID: 16544313
-
[EAU guidelines on prostate cancer. Part II: treatment of advanced, relapsing, and castration-resistant prostate cancer].Actas Urol Esp. 2011 Nov-Dec;35(10):565-79. doi: 10.1016/j.acuro.2011.03.011. Epub 2011 Jul 14. Actas Urol Esp. 2011. PMID: 21757258 Spanish.
Cited by
-
CRISPR/Cas9 Technology Providing the Therapeutic Landscape of Metastatic Prostate Cancer.Pharmaceuticals (Basel). 2024 Nov 26;17(12):1589. doi: 10.3390/ph17121589. Pharmaceuticals (Basel). 2024. PMID: 39770431 Free PMC article. Review.
-
Integrative genomic analysis identifies DPP4 inhibition as a modulator of FGF17 and PDGFRA downregulation and PI3K/Akt pathway suppression leading to apoptosis.Front Pharmacol. 2025 Jul 22;16:1606914. doi: 10.3389/fphar.2025.1606914. eCollection 2025. Front Pharmacol. 2025. PMID: 40766751 Free PMC article.
-
Medicaid Expansion and Survival Outcomes Among Men With Prostate Cancer.Cureus. 2025 Jan 14;17(1):e77434. doi: 10.7759/cureus.77434. eCollection 2025 Jan. Cureus. 2025. PMID: 39822252 Free PMC article.
-
Unlocking the Potential of Gracilaria chilensis Against Prostate Cancer.Plants (Basel). 2025 Jul 31;14(15):2352. doi: 10.3390/plants14152352. Plants (Basel). 2025. PMID: 40805701 Free PMC article.
-
Reversing the "cold" tumor microenvironment: the role of neoantigen vaccines in prostate cancer.J Transl Med. 2025 Jul 25;23(1):835. doi: 10.1186/s12967-025-06867-8. J Transl Med. 2025. PMID: 40713775 Free PMC article.
References
-
- Tolis G., Ackman D., Stellos A., Mehta A., Labrie F., Fazekas A.T., Comaru-Schally A.M., Schally A.V. Tumor growth inhibition in patients with prostatic carcinoma treated with luteinizing hormone-releasing hormone agonists. Proc. Natl. Acad. Sci. USA. 1982;79:1658–1662. doi: 10.1073/pnas.79.5.1658. - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
