

Development and Validation of a Nomogram to Predict Overall Survival in Stage I-III Colorectal Cancer Patients after Radical Resection with Normal Preoperative Serum Carcinoembryonic Antigen
- PMID: 38067346
- PMCID: PMC10705739
- DOI: 10.3390/cancers15235643
Development and Validation of a Nomogram to Predict Overall Survival in Stage I-III Colorectal Cancer Patients after Radical Resection with Normal Preoperative Serum Carcinoembryonic Antigen
Abstract
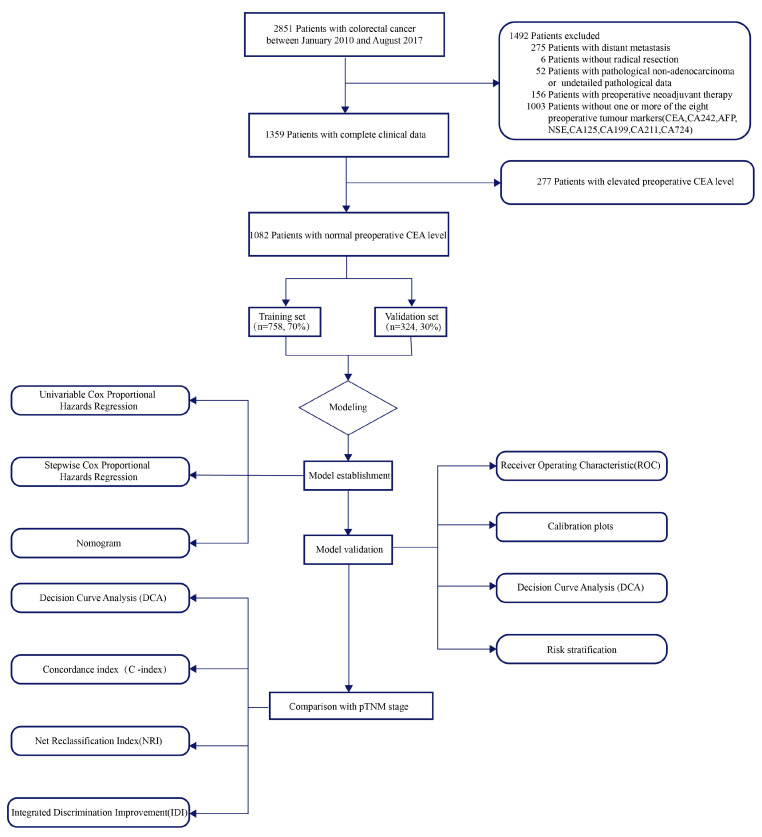
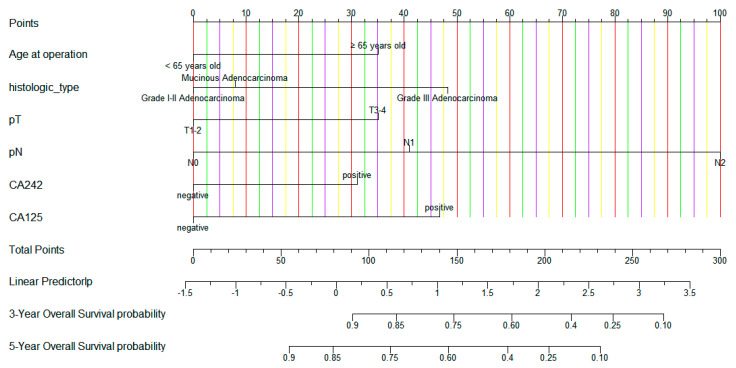
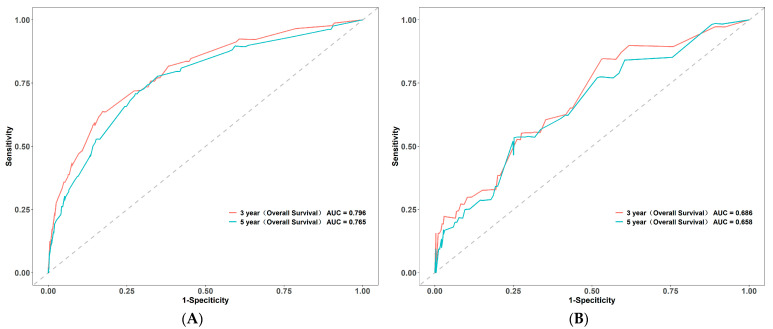
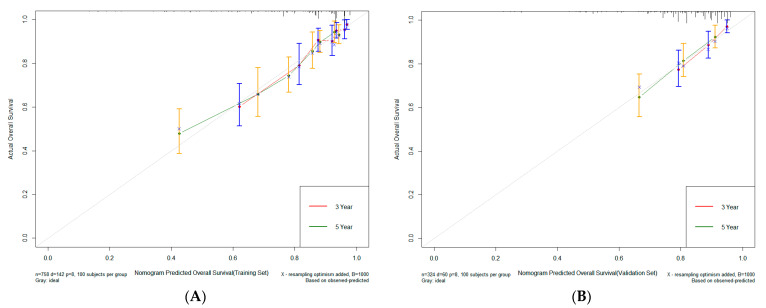
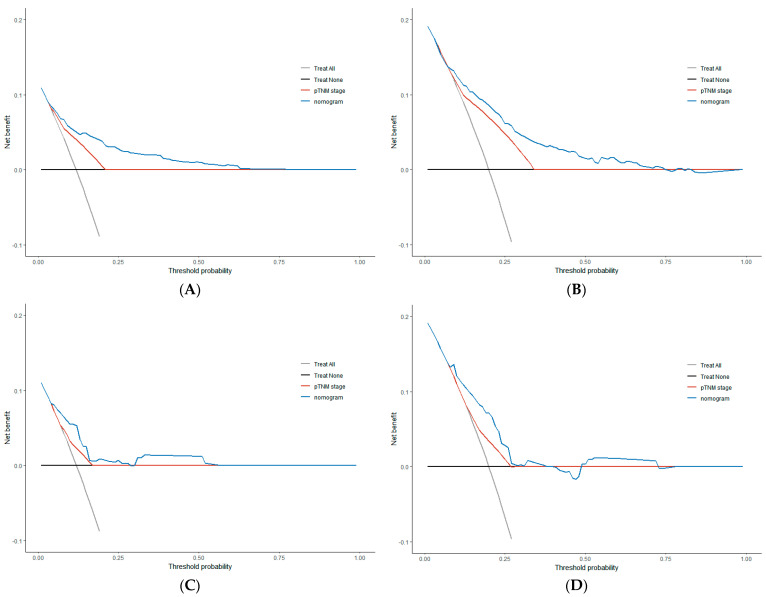
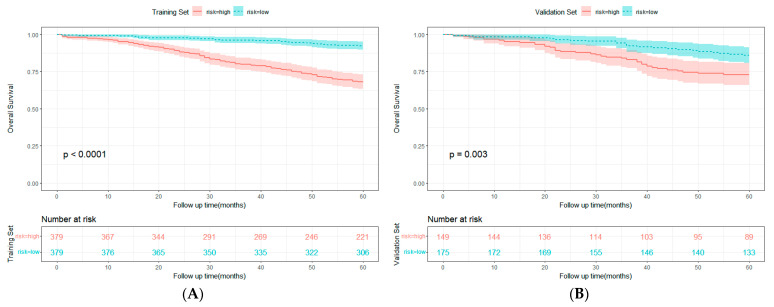
We aimed to develop a clinical predictive model for predicting the overall survival (OS) in stage I-III CRC patients after radical resection with normal preoperative CEA. This study included 1082 consecutive patients. They were further divided into a training set (70%) and a validation set (30%). The selection of variables for the model was informed by the Akaike information criterion. After that, the clinical predictive model was constructed, evaluated, and validated. The net reclassification index (NRI) and integrated discrimination improvement (IDI) were employed to compare the models. Age, histologic type, pT stage, pN stage, carbohydrate antigen 242 (CA242), and carbohydrate antigen 125 (CA125) were selected to establish a clinical prediction model for OS. The concordance index (C-index) (0.748 for the training set and 0.702 for the validation set) indicated that the nomogram had good discrimination ability. The decision curve analysis highlighted that the model has superior efficiency in clinical decision-making. NRI and IDI showed that the established nomogram markedly outperformed the TNM stage. The new clinical prediction model was notably superior to the AJCC 8th TNM stage, and it can be used to accurately assess the OS of stage I-III CRC patients undergoing radical resection with normal preoperative CEA.
Keywords: CA125; CA242; colorectal cancer; nomogram; overall survival.
Conflict of interest statement
The authors declare that they have no known competing financial interest or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Development and validation of nomograms based on pre-/post-operative CEA and CA19-9 for survival predicting in stage I-III colorectal cancer patients after radical resection.Front Oncol. 2024 Oct 11;14:1402847. doi: 10.3389/fonc.2024.1402847. eCollection 2024. Front Oncol. 2024. PMID: 39464705 Free PMC article.
-
Development and validation of a prognostic nomogram for colorectal cancer after surgery.World J Clin Cases. 2021 Jul 26;9(21):5860-5872. doi: 10.12998/wjcc.v9.i21.5860. World J Clin Cases. 2021. PMID: 34368305 Free PMC article.
-
Clinical Significance of and Predictive Risk Factors for the Postoperative Elevation of Carcinoembryonic Antigen in Patients With Non-Metastatic Colorectal Cancer.Front Oncol. 2021 Oct 7;11:741309. doi: 10.3389/fonc.2021.741309. eCollection 2021. Front Oncol. 2021. PMID: 34692522 Free PMC article.
-
Preoperative Systemic Immune-Inflammation Index (SII) as a Superior Predictor of Long-Term Survival Outcome in Patients With Stage I-II Gastric Cancer After Radical Surgery.Front Oncol. 2022 Feb 28;12:829689. doi: 10.3389/fonc.2022.829689. eCollection 2022. Front Oncol. 2022. PMID: 35296020 Free PMC article.
-
[Analysis of related factors of prognosis after surgical treatment of patients with non-metastatic colorectal cancer and construction of a normagram prediction model].Zhonghua Zhong Liu Za Zhi. 2022 Feb 23;44(2):167-172. doi: 10.3760/cma.j.cn112152-20200321-00244. Zhonghua Zhong Liu Za Zhi. 2022. PMID: 35184461 Chinese.
Cited by
-
OncoE25: an AI model for predicting postoperative prognosis in early-onset stage I-III colon and rectal cancer-a population-based study using SEER with dual-center cohort validation.J Transl Med. 2025 Jun 22;23(1):695. doi: 10.1186/s12967-025-06663-4. J Transl Med. 2025. PMID: 40545536 Free PMC article.
-
Predicting treatment failure in stage III colon cancer patients after radical surgery.Front Oncol. 2024 May 16;14:1397468. doi: 10.3389/fonc.2024.1397468. eCollection 2024. Front Oncol. 2024. PMID: 38817900 Free PMC article.
References
-
- Takagawa R., Fujii S., Ohta M., Nagano Y., Kunisaki C., Yamagishi S., Osada S., Ichikawa Y., Shimada H. Preoperative serum carcinoembryonic antigen level as a predictive factor of recurrence after curative resection of colorectal cancer. Ann. Surg. Oncol. 2008;15:3433–3439. doi: 10.1245/s10434-008-0168-8. - DOI - PubMed
-
- Park J.W., Lim S.B., Kim D.Y., Jung K.H., Hong Y.S., Chang H.J., Choi H.S., Jeong S.Y. Carcinoembryonic antigen as a predictor of pathologic response and a prognostic factor in locally advanced rectal cancer patients treated with preoperative chemoradiotherapy and surgery. Int. J. Radiat. Oncol. Biol. Phys. 2009;74:810–817. doi: 10.1016/j.ijrobp.2008.08.057. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
