

Local MRI before and after Tumor Resection in Neuroblastoma: Impact of Residual Disease on Event Free Survival
- PMID: 38068349
- PMCID: PMC10707530
- DOI: 10.3390/jcm12237297
Local MRI before and after Tumor Resection in Neuroblastoma: Impact of Residual Disease on Event Free Survival
Abstract
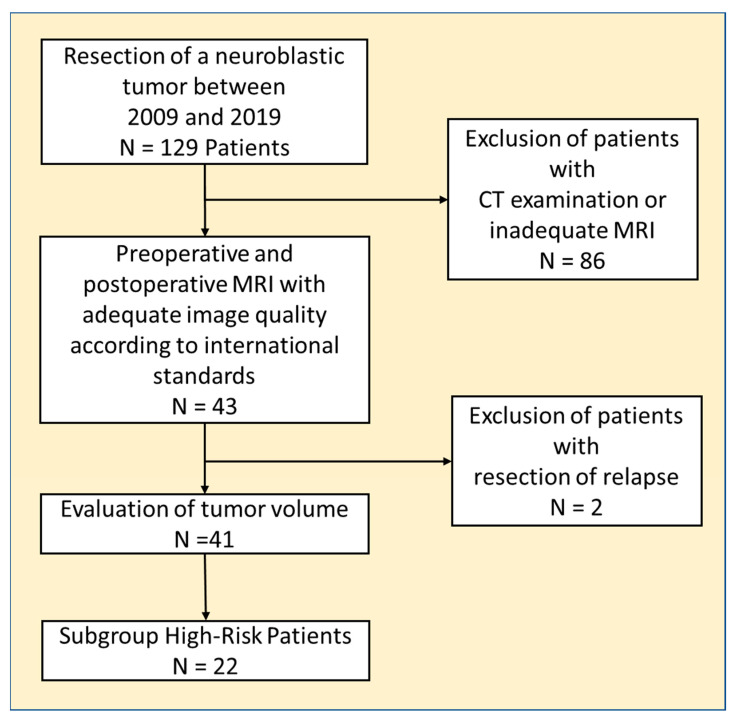
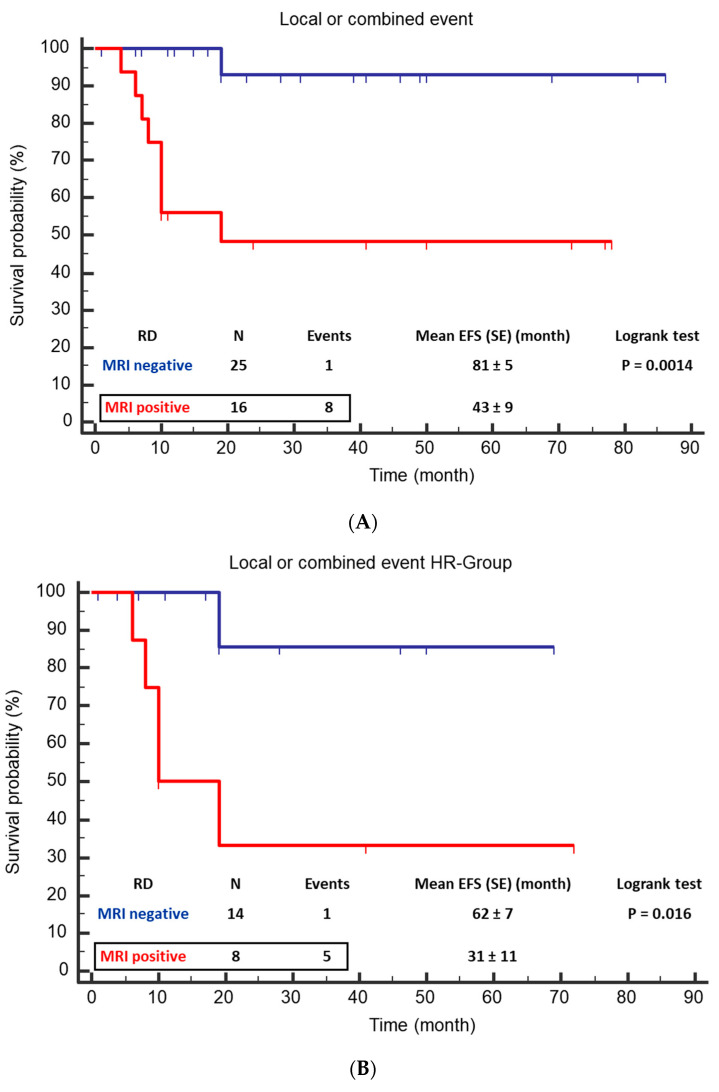
(1) Background: The study aimed to investigate the influence of MRI-defined residual disease on local tumor control after resection of neuroblastic tumors in patients without routine adjuvant radiotherapy. (2) Methods: Patients, who underwent tumor resection between 2009 and 2019 and received a pre- and postoperative MRI, were included in this retrospective single-center study. Measurement of residual disease (RD) was performed using standardized criteria. Primary endpoint was the local or combined (local and metastatic) event free survival (EFS). (3) Results: Forty-one patients (20 female) with median age of 39 months were analyzed. Risk group analysis showed eleven low-, eight intermediate-, and twenty-two high-risk patients (LR, IR, HR). RD was found in 16 cases by MRI. A local or combined relapse or progression was found in nine patients of whom eight patients had RD (p = 0.0004). From the six patients with local or combined relapse in the HR group, five had RD (p = 0.005). Only one of 25 patients without RD had a local event. Mean EFS (month) was significantly higher if MRI showed no residual tumor (81 ± 5 vs. 43 ± 9; p = 0.0014) for the total cohort and the HR subgroup (62 ± 7 vs. 31 ± 11; p = 0.016). (4) Conclusions: In our series, evidence of residual tumor, detectable by MRI, was associated with insufficient local control, resulting in relapses or local progression in 50% of patients. Only one of the patients without residual tumor had a local relapse.
Keywords: EFS; MRI; high-risk neuroblastoma; irradiation; residual tumor; surgical resection.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Ries L.A.G., Smith M.A., Gurney J., Linet M., Tamra T., Young J., Bunin G. Cancer Incidence and Survival among Children and Adolescents: United States SEER Program 1975–1995. National Cancer Institute; Rockville, MD, USA: 1999.
-
- Brisse H.J., McCarville M.B., Granata C., Krug K.B., Wootton-Gorges S.L., Kanegawa K., Giammarile F., Schmidt M., Shulkin B.L., Matthay K.K., et al. Guidelines for imaging and staging of neuroblastic tumors: Consensus report from the International Neuroblastoma Risk Group Project. Radiology. 2011;261:243–257. doi: 10.1148/radiol.11101352. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
