

Ketogenic diet therapy for pediatric epilepsy is associated with alterations in the human gut microbiome that confer seizure resistance in mice
- PMID: 38070135
- PMCID: PMC10769314
- DOI: 10.1016/j.celrep.2023.113521
Ketogenic diet therapy for pediatric epilepsy is associated with alterations in the human gut microbiome that confer seizure resistance in mice
Abstract
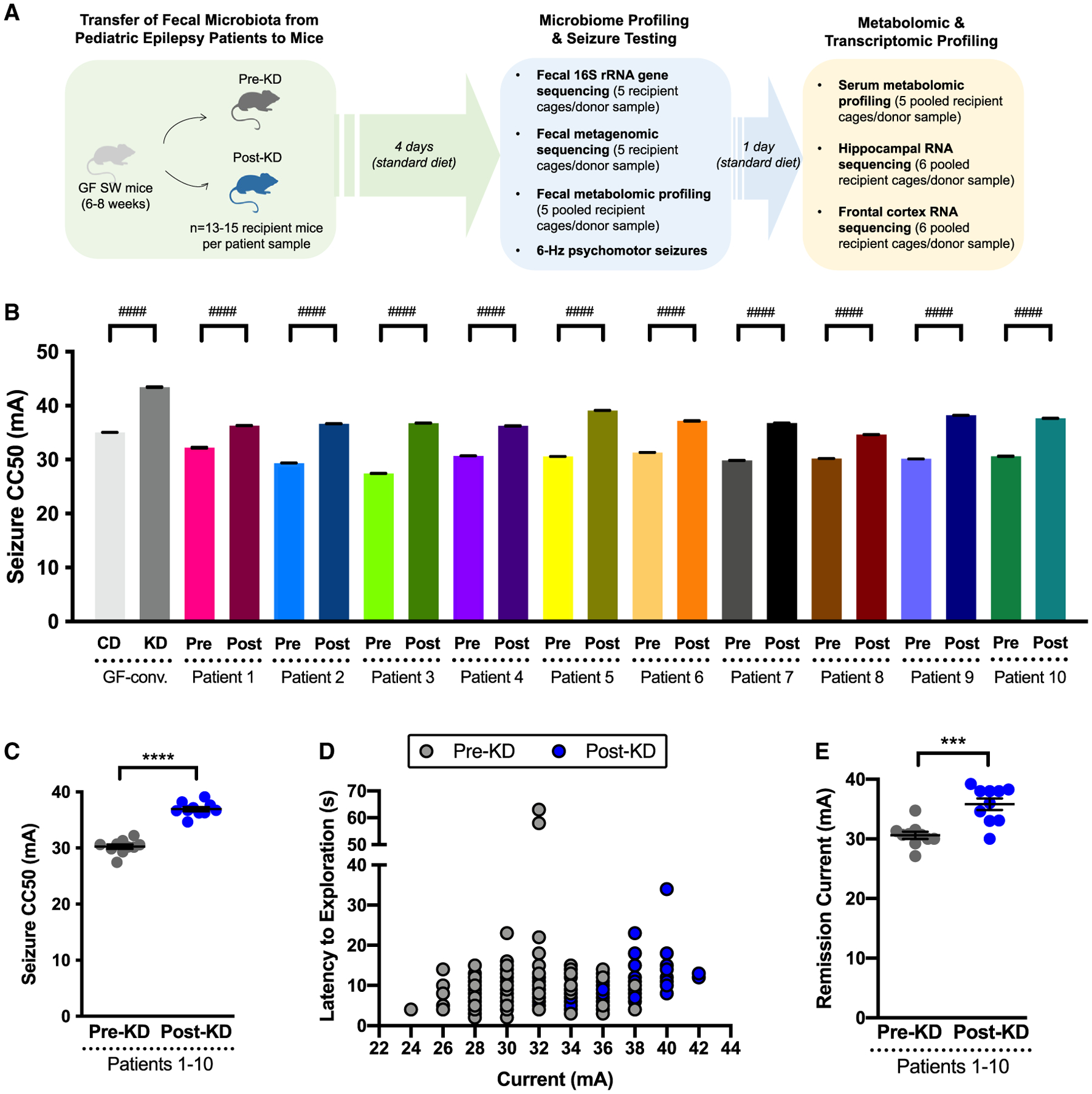
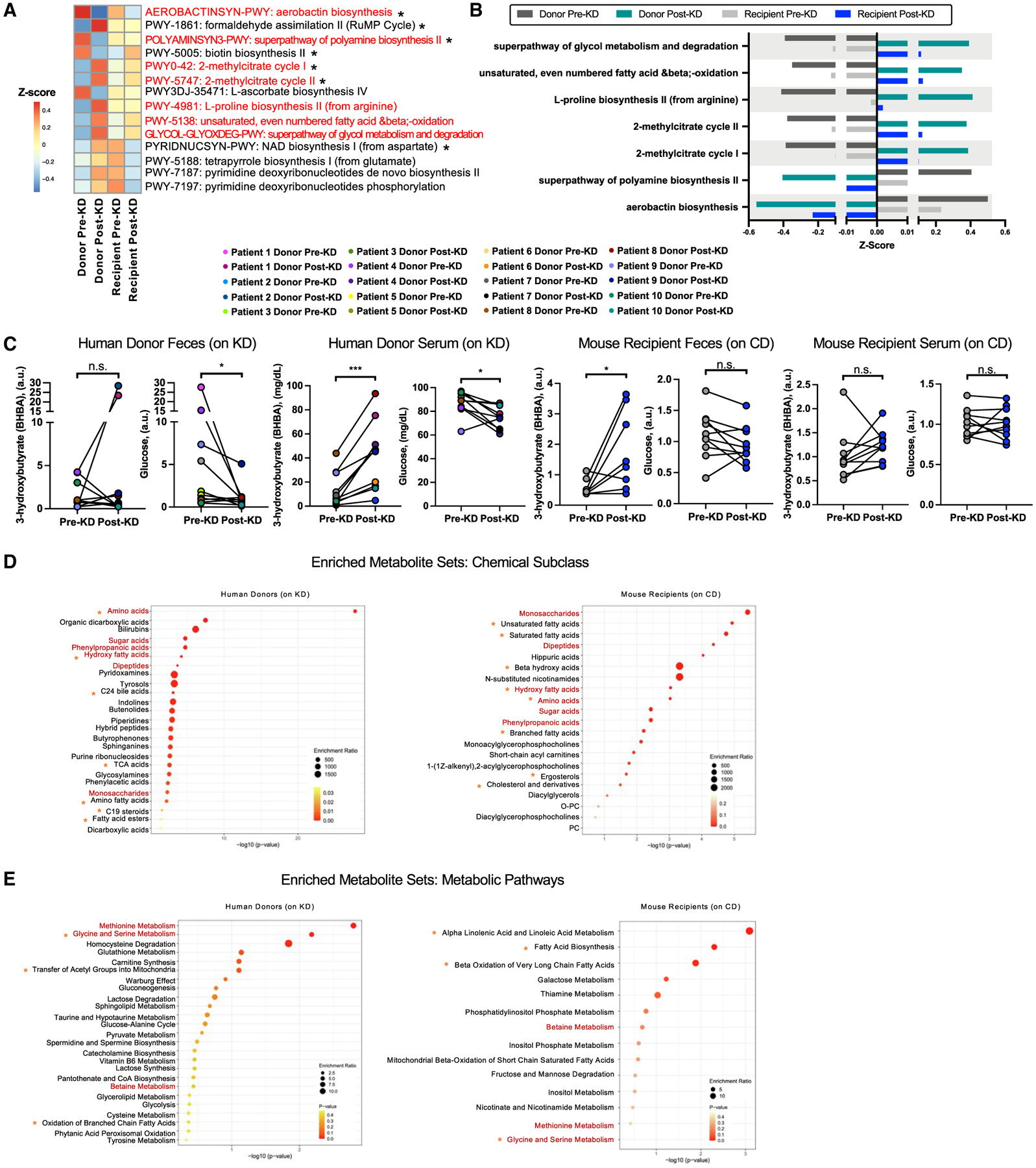
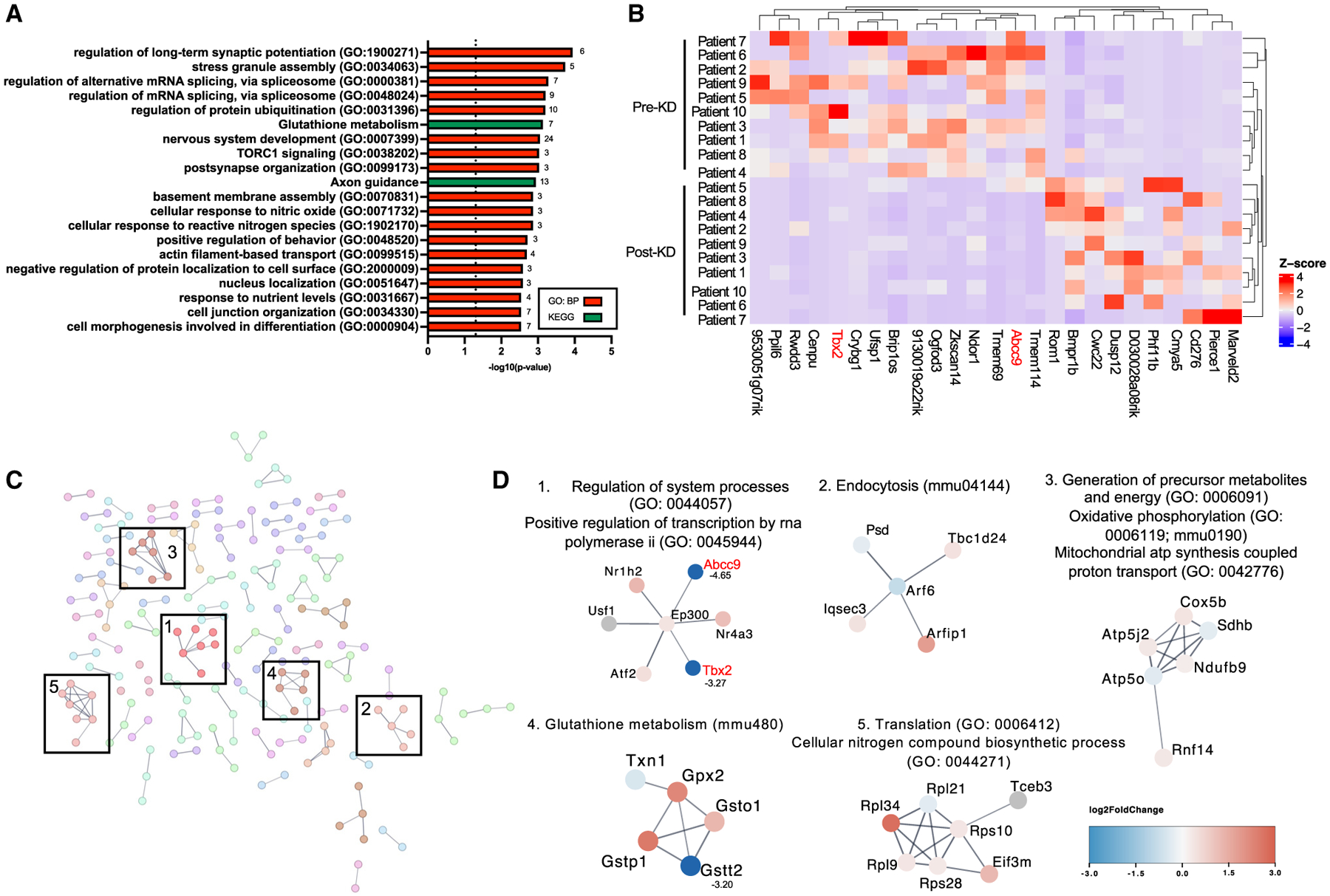
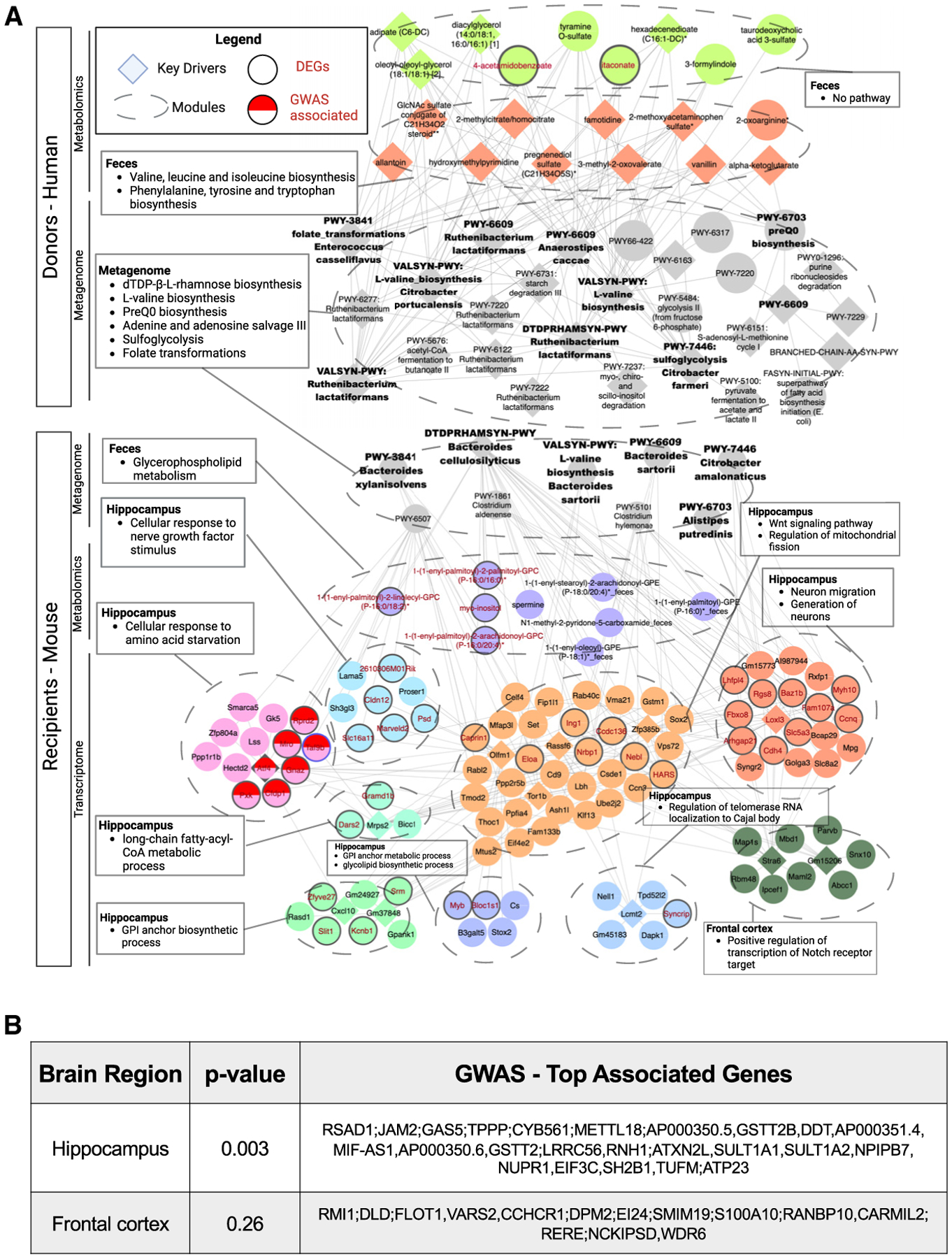
The gut microbiome modulates seizure susceptibility and the anti-seizure effects of the ketogenic diet (KD) in animal models, but whether these relationships translate to KD therapies for human epilepsy is unclear. We find that the clinical KD alters gut microbial function in children with refractory epilepsy. Colonizing mice with KD-associated microbes promotes seizure resistance relative to matched pre-treatment controls. Select metagenomic and metabolomic features, including those related to anaplerosis, fatty acid β-oxidation, and amino acid metabolism, are seen with human KD therapy and preserved upon microbiome transfer to mice. Mice colonized with KD-associated gut microbes exhibit altered hippocampal transcriptomes, including pathways related to ATP synthesis, glutathione metabolism, and oxidative phosphorylation, and are linked to susceptibility genes identified in human epilepsy. Our findings reveal key microbial functions that are altered by KD therapies for pediatric epilepsy and linked to microbiome-induced alterations in brain gene expression and seizure protection in mice.
Keywords: CP: Microbiology; CP: Neuroscience; epilepsy; ketogenic diet; microbiome; seizure.
Copyright © 2023 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests The findings are the subject of UCLA provisional patent application US 63/285,267. E.Y.H. has financial interests in Bloom Science.
Figures
Comment in
-
Fecal transfers from children on the ketogenic diet mimic the anti-seizure effect in mice.Cell Rep. 2023 Dec 26;42(12):113570. doi: 10.1016/j.celrep.2023.113570. Epub 2023 Dec 8. Cell Rep. 2023. PMID: 38070136
References
-
- Coppola G, Veggiotti P, Cusmai R, Bertoli S, Cardinali S, Dionisi-Vici C, Elia M, Lispi ML, Sarnelli C, Tagliabue A, et al. (2002). The ketogenic diet in children, adolescents and young adults with refractory epilepsy: An Italian multicentric experience. Epilepsy Res. 48, 221–227. - PubMed
-
- Freeman JM, Vining EP, Pillas DJ, Pyzik PL, Casey JC, and Kelly LM (1998). The efficacy of the ketogenic diet - 1998: A prospective evaluation of intervention in 150 children. Pediatrics 102, 1358–1363. - PubMed
-
- Kang HC, Kim YJ, Kim DW, and Kim HD (2005). Efficacy and safety of the ketogenic diet for intractable childhood epilepsy: Korean multicentric experience. Epilepsia 46, 272–279. - PubMed
-
- Neal EG, Chaffe H, Schwartz RH, Lawson MS, Edwards N, Fitz-simmons G, Whitney A, and Cross JH (2008). The ketogenic diet for the treatment of childhood epilepsy: a randomised controlled trial. Lancet Neurol. 7, 500–506. - PubMed
-
- Kossoff EH, Zupec-Kania BA, Auvin S, Ballaban-Gil KR, Christina Bergqvist AG, Blackford R, Buchhalter JR, Caraballo RH, Cross JH, Dahlin MG, et al. (2018). Optimal clinical management of children receiving dietary therapies for epilepsy: Updated recommendations of the International Ketogenic Diet Study Group. Epilepsia Open 3, 175–192. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
