

SARS-CoV-2 receptor ACE2 is upregulated by fatty acids in human MASH
- PMID: 38074511
- PMCID: PMC10698276
- DOI: 10.1016/j.jhepr.2023.100936
SARS-CoV-2 receptor ACE2 is upregulated by fatty acids in human MASH
Abstract
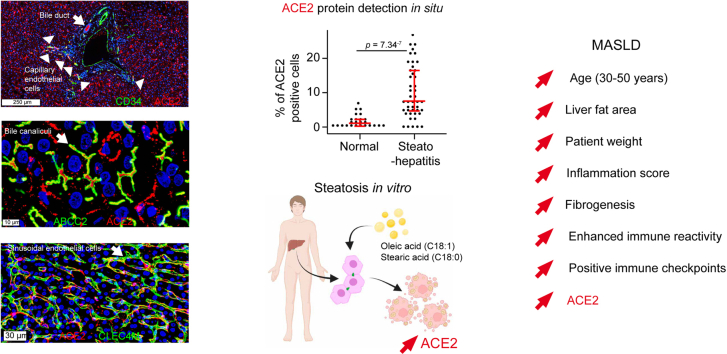
Background & aims: Metabolic dysfunction-associated steatotic liver disease (MASLD) results in steatosis, inflammation (steatohepatitis), and fibrosis. Patients with MASLD more likely develop liver injury in coronavirus disease 2019 (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). As viral RNA has been identified in liver tissues, we studied expression levels and cellular sources of the viral receptor angiotensin-converting enzyme 2 (ACE2) and coreceptors in MASLD and fibroinflammatory liver diseases.
Methods: We built a transcriptomic MASLD meta-dataset (N = 243) to study SARS-CoV-2 receptor expression and verified results in 161 additional cases of fibroinflammatory liver diseases. We assessed the fibroinflammatory microenvironment by deconvoluting immune cell populations. We studied the cellular sources of ACE2 by multiplex immunohistochemistry followed by high-resolution confocal microscopy (N = 9 fatty livers; N = 7 controls), meta-analysis of two single-cell RNA sequencing datasets (N = 5 cirrhotic livers; N = 14 normal livers), and bulk transcriptomics from 745 primary cell samples. In vitro, we tested ACE2 mRNA expression in primary human hepatocytes treated with inflammatory cytokines, bacterial lipopolysaccharides, or long-chain fatty acids.
Results: We detected ACE2 at the apical and basal poles of hepatocyte chords, in CLEC4M+ liver sinusoidal endothelial cells, the lumen of ABCC2+ bile canaliculi, HepPar-1+-TMPRSS2+ hepatocytes, cholangiocytes, and CD34+ capillary vessels. ACE2 steeply increased between 30 and 50 years of age; was related to liver fat area, inflammation, high immune reactivity, and fibrogenesis; and was upregulated in steatohepatitis. Although ACE2 mRNA was unmodified in alcoholic or viral hepatitis, it was upregulated in fibroinflammatory livers from overweight patients. In vitro, treatment of primary human hepatocytes with inflammatory cytokines alone downregulated but long chain fatty acids upregulated ACE2 mRNA expression.
Conclusions: Lipid overload in fatty liver disease leads to an increased availability of ACE2 receptors.
Impact and implications: COVID-19 can be a deadly disease in vulnerable individuals. Patients with fatty liver disease are at a higher risk of experiencing severe COVID-19 and liver injury. Recent studies have indicated that one of the reasons for this vulnerability is the presence of a key cell surface protein called ACE2, which serves as the main SARS-CoV-2 virus receptor. We describe the cellular sources of ACE2 in the liver. In patients with fatty liver disease, ACE2 levels increase with age, liver fat content, fibroinflammatory changes, enhanced positive immune checkpoint levels, and innate immune reactivity. Moreover, we show that long chain fatty acids can induce ACE2 expression in primary human hepatocytes. Understanding the cellular sources of ACE2 in the liver and the factors that influence its availability is crucial. This knowledge will guide further research and help protect potentially vulnerable patients through timely vaccination boosters, dietary adjustments, and improved hygiene practices.
Keywords: CLEC4M; DC-SIGNR; DPP4; MAFLD; Metabolic syndrome; Metabolism; NAFLD; NASH; Oleic acid; SARS-CoV-2; Stearic acid; TMPRSS2.
© 2023 The Author(s).
Conflict of interest statement
The authors of this study declare that they do not have any conflict of interest. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures







References
-
- Eslam M., Sanyal A.J., George J. MAFLD: a consensus-driven proposed nomenclature for metabolic associated fatty liver disease. Gastroenterology. 2020;158:1999–2014.e1991. - PubMed
-
- Eslam M., Newsome P.N., Sarin S.K., et al. A new definition for metabolic dysfunction-associated fatty liver disease: an international expert consensus statement. J Hepatol. 2020;73:202–209. - PubMed
-
- Rinella M.E., Lazarus J.V., Ratziu V., et al. A multi-society Delphi consensus statement on new fatty liver disease nomenclature. J Hepatol. 2023 in press. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
