

Molecular characterization of the new clinical entity associated with congenital adrenal hyperplasia: the CAH-X syndrome in the Spanish population
- PMID: 38075167
- PMCID: PMC10701499
- DOI: 10.1515/almed-2023-0071
Molecular characterization of the new clinical entity associated with congenital adrenal hyperplasia: the CAH-X syndrome in the Spanish population
Abstract
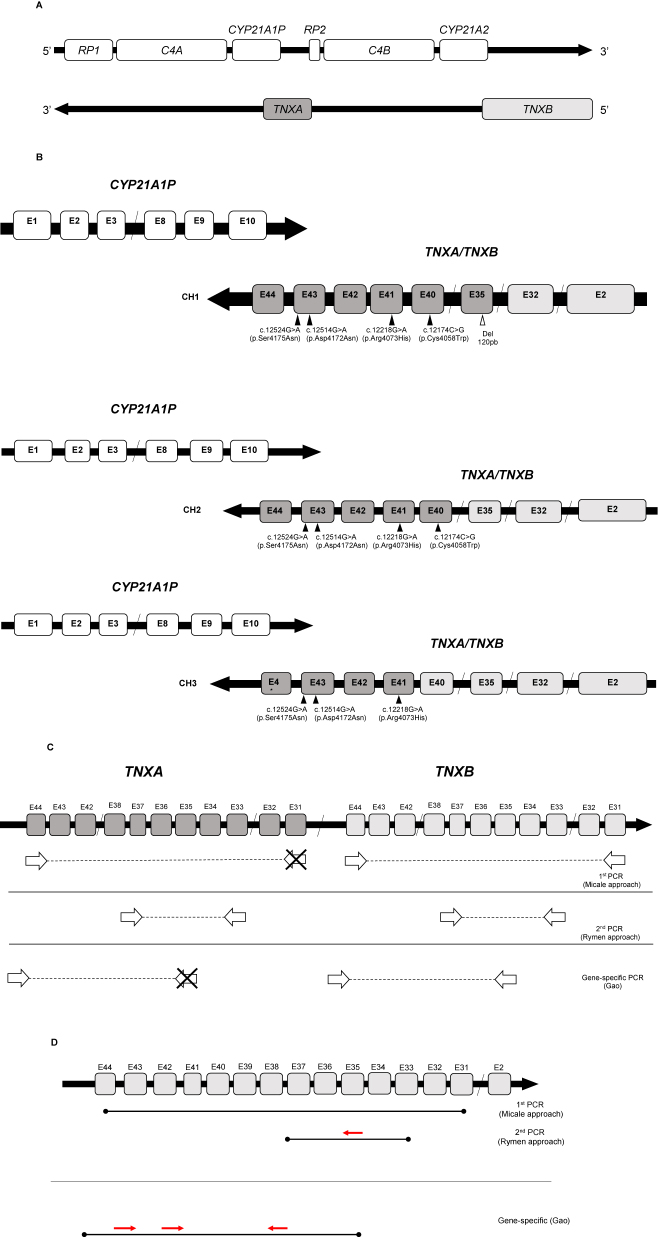
Objectives: The chimeras causing the CAH-X syndrome (SCAH-X) result from recombination between CYP21A2-TNXB and their respective pseudogenes (CYP21A1P-TNXA). The clinical manifestations of this syndrome include congenital adrenal hyperplasia (CAH) and Ehlers-Danlos syndrome (EDS). Since SCAH-X has been recently described, the number of publications available is limited. The objective of this study was to set up a molecular approach and a screening algorithm for detecting CAH-X chimeras, determine their frequency and distribution in the Spanish population, and assess their clinical pattern of occurrence in a group of patients.
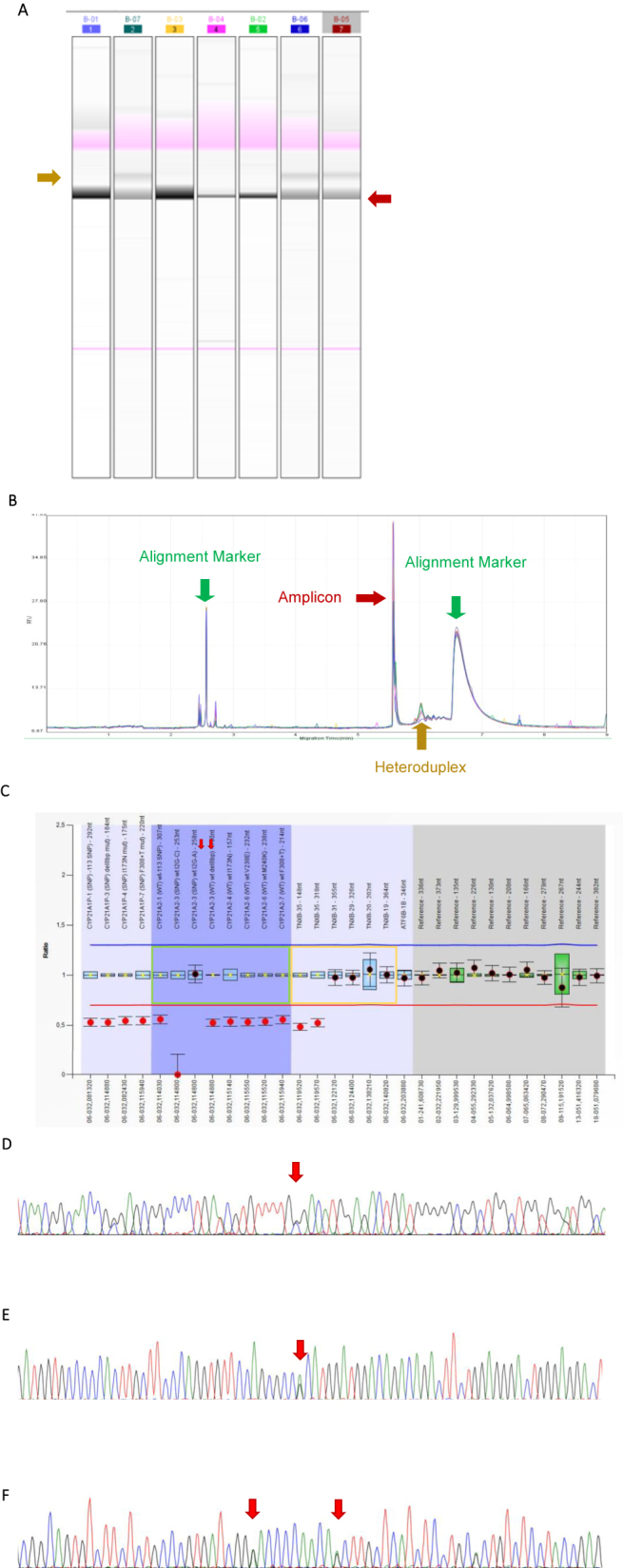
Methods: A total of 186 patients were eligible for CAH-X molecular genetic testing. Testing included MLPA, heterodimer detection by capillary gel electrophoresis, and sequencing of exons 40, 41, and 43 of TNXB. A review was performed of the medical history of 20 patients from three hospitals of reference and the signs and symptoms of EDS they exhibited.
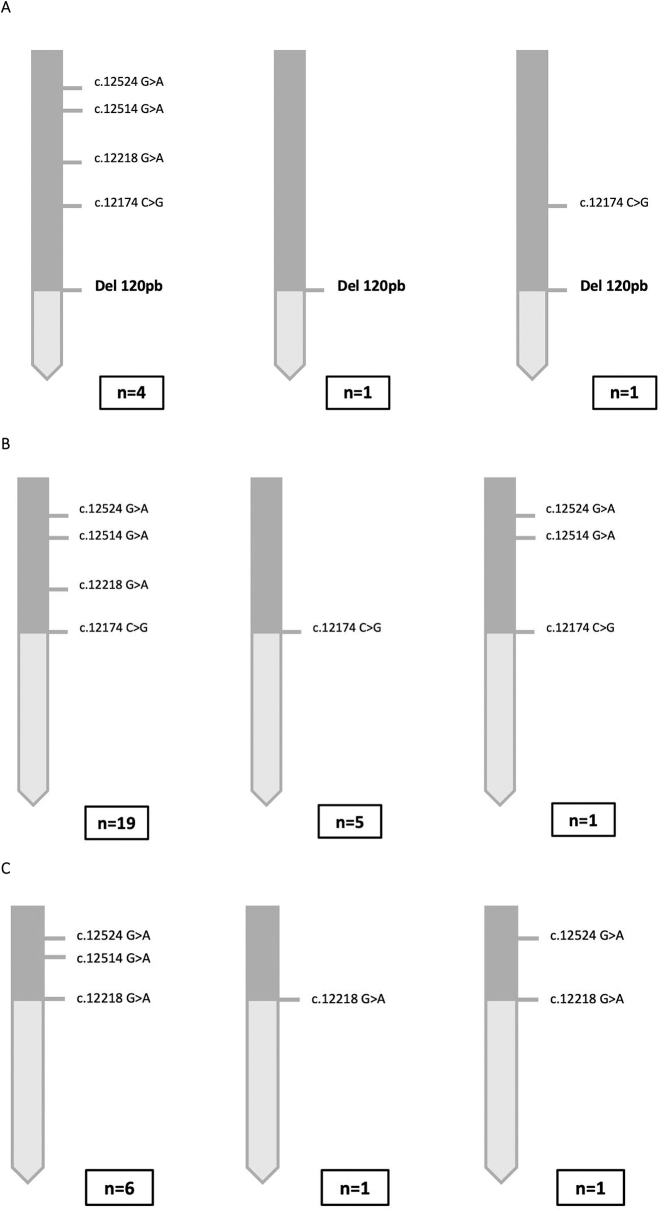
Results: In total, 78 CAH patients were carriers of CAH-X chimeras (41.9 %). Forty-six patients were carriers of CH1 (24.7 %), 24 of CH2 (12.9 %), and 8 of CH3 (4.3 %), with a heterogeneous geographical distribution. Seven (35 %) of the 20 carriers of a CAH-X chimera who underwent clinical examination experienced clinical manifestations of EDS.
Conclusions: The impact of SCAH-X in the Spanish population was assessed by genetic testing. In the light of the clinical pattern of occurrence and significant prevalence of SCAH-X in the Spanish population, early diagnosis of this entity is essential for an appropriate follow-up of clinical manifestations.
Keywords: CAH-X syndrome; CYP21A2; TNXB; congenital adrenal hyperplasia; hypermobility-type Ehlers–Danlos syndrome; tenascin.
© 2023 the author(s), published by De Gruyter, Berlin/Boston.
Conflict of interest statement
Competing interests: The authors state no conflict of interest.
Figures
References
-
- Grau G, Vela A, Estévez AR, Rica I. Insuficiencia suprarrenal. Protoc diagn ter pediatr. Madrid: Exlibris; 2019. pp. 205–15.
-
- Ezquieta Zubicaray B. Barcelona: Educación Continuada Laboratorio Clínico. 2013. Hiperplasia Suprarrenal Congénita. Forma neonatal con pérdida salina y diagnóstico previo de pseudohipoaldosteronismo. En: Genética Molecular aplicada al diagnóstico de enfermedades hereditarias; pp. 75–94.
-
- Rodríguez A, Ezquieta B, Labarta JI, Clemente M, Espino R, Rodriguez A, et al. Recomendaciones para el diagnóstico y tratamiento de pacientes con formas clásicas de hiperplasia suprarrenal congénita por déficit de 21-hidroxilasa. Pediatr. 2017;87:116.e1–10. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous